Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.
If you have pain shooting from your backside down the back of your leg, someone has probably already told you it’s “sciatica.” Maybe a friend, maybe the internet, maybe a search bar that pattern-matched your symptoms in half a second. But here’s the catch: not all leg pain that feels like sciatica is coming from your spine. Understanding piriformis syndrome vs true sciatica matters because the two can look almost identical from the outside while behaving very differently underneath — and that difference quietly changes what you should do about it.
Both involve the sciatic nerve. Both can send pain into the buttock and down the leg. Both can make sitting miserable. The split comes down to where the nerve is being irritated — at its root near the spine, or further downstream as it passes through a deep muscle in the buttock. Get that wrong and you can spend months stretching a muscle that was never the problem, or bracing a spine that was never the cause.
Key Takeaways
- True sciatica is leg pain caused by irritation or compression of a lumbar nerve root (most often L5 or S1) near the spine — usually from a disc or stenosis. The pain typically follows a clear nerve path and is often paired with numbness, tingling, or weakness.
- Piriformis syndrome is one cause of a “sciatica-like” pattern where the sciatic nerve is irritated outside the spine, in the deep buttock — the pain is more buttock-dominant and tied to hip position and prolonged sitting.
- The single most useful question: Does your pain start at your back, or in the middle of your buttock?
- Most leg pain — from either source — improves with conservative care over weeks. Imaging is rarely the first step.
- A short list of red flags (bowel/bladder changes, saddle numbness, progressive weakness, fever) overrides everything below and needs urgent assessment.
Piriformis Syndrome vs True Sciatica: What’s the Real Difference?
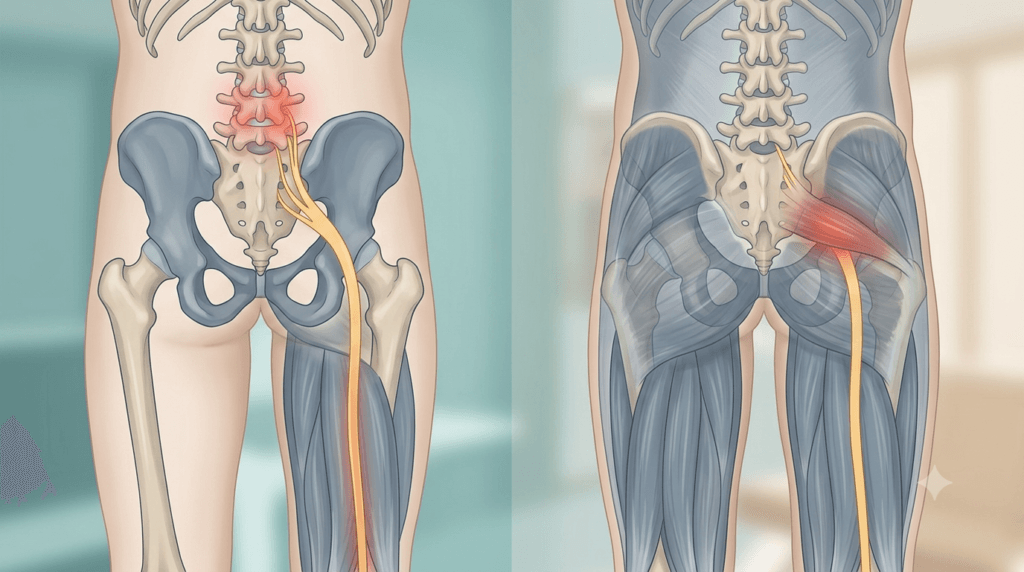
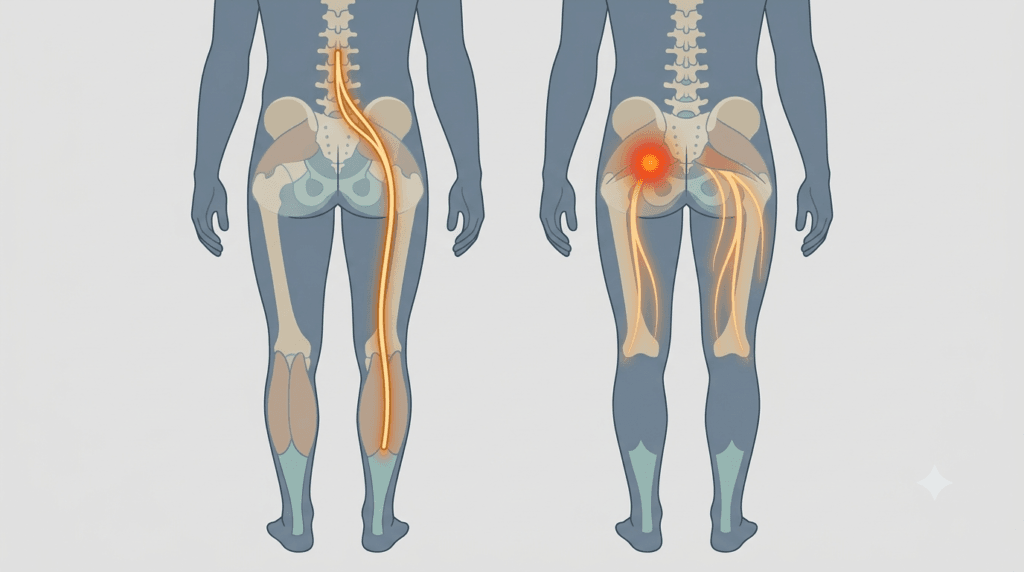
The real difference is location of the problem, not location of the pain. True sciatica is a radicular problem — the sciatic nerve’s roots are pinched where they exit the lower spine, so pain originates near the back and travels down a specific nerve line. Piriformis syndrome is a non-spinal sciatic irritation — the nerve is squeezed by the piriformis muscle deep in the buttock, so the buttock is usually the loudest spot.
The sciatic nerve is the thickest nerve in the body. It forms from roots in your lower back, threads through the pelvis, and passes right next to (and in some people, straight through) the piriformis — a small, deep muscle that rotates your hip outward. “Sciatica” technically just means irritation of that nerve anywhere along its path. So strictly speaking, piriformis syndrome can produce sciatica. What we mean by “true sciatica” in everyday language is radicular pain from the spine, and that’s the comparison most people are actually asking about.
Piriformis syndrome belongs to a broader category clinicians now call deep gluteal syndrome — a group of non-discogenic causes of sciatic irritation that mimic spinal nerve root pain and are notoriously easy to miss (Park et al., Bone & Joint Journal, 2020).
How Are the Symptom Patterns Different Day to Day?
Day to day, the clearest tell is where the pain lives and what provokes it. Spinal sciatica usually anchors at the back or buttock and shoots below the knee in a defined line, often worse with coughing, sneezing, bending, or sitting that loads the disc. Piriformis-type pain centers in the mid-buttock, flares with prolonged sitting (especially on a hard surface or a wallet), and eases when you stand and walk it off.
Neither rule is absolute — bodies don’t read textbooks — but the patterns below hold up well enough to guide your next move. This is also where it helps to separate true nerve pain from referred ache; a related read on telling hip-driven pain from back-driven pain covers that overlap in more depth.
| Feature | True (Spinal) Sciatica | Piriformis Syndrome |
|---|---|---|
| Where it starts | Lower back or upper buttock | Deep in the middle of the buttock |
| How far it travels | Often below the knee, into calf or foot, in a clear line | Often stops at the back of the thigh; may reach the calf |
| Worse with | Coughing, sneezing, bending forward, sitting that rounds the spine | Prolonged sitting, climbing stairs, sitting on a hard surface or wallet |
| Better with | Lying down, gentle position changes, walking (sometimes) | Standing up, walking, getting off the seat |
| Numbness/tingling | Common, often in a specific toe or foot region | Possible but vaguer, more buttock/thigh |
| Tenderness | Usually not tender to press the buttock | Often tender to press deep in the mid-buttock |
| Onset | Frequently linked to a lifting or bending event | More often gradual, linked to sitting, running, or a change in activity |
A useful mental shortcut from years in clinic: spinal sciatica tends to be a “line” of pain; piriformis pain tends to be a “spot” that radiates. That systematic-review work backs this up — piriformis presentations cluster around buttock pain, pain worse on sitting, tenderness near the greater sciatic notch, and reproduction of pain with movements that stretch the muscle (Hopayian & Danielyan, Eur J Orthop Surg Traumatol, 2018).
Why Do the Two Get Confused So Often?
They get confused because the sciatic nerve is the shared messenger, and the message (leg pain) can read the same regardless of where it was triggered. The body can only complain in so many ways. A nerve irritated at the root and a nerve squeezed in the buttock both broadcast pain down the same wiring.
A few other reasons the labels blur:
- “Sciatica” is a symptom, not a diagnosis. It describes a pain pattern, not a cause. Two people with identical leg pain can have completely different sources.
- Imaging muddies the water. Plenty of pain-free adults have disc bulges on MRI. So a scan showing a disc issue doesn’t automatically mean the disc is causing your buttock pain — it may be an innocent bystander.
- Tight glutes confuse the picture. Buttock tightness and hip stiffness can ride along with either condition, which is why people often chase the muscle when the spine is the driver, or vice versa. There’s a fuller breakdown of how tight glutes feed into lower back and buttock pain if that’s part of your picture.
What Are the Red Flags That Change Everything?
Some symptoms aren’t about telling piriformis from sciatica — they’re about ruling out something serious, and they take priority over every other consideration here. If any of the following are present, this article stops being your guide and prompt in-person assessment becomes the priority.
Seek urgent care if you have:
- Loss of bladder or bowel control, or new difficulty starting/stopping urination
- Numbness around the groin, inner thighs, or saddle area (the region that contacts a bike seat)
- Rapidly worsening weakness in the leg or foot — for example, a foot that’s starting to drag
- Numbness or weakness in both legs
- Fever, unexplained weight loss, or night pain alongside the back/leg pain
- Severe pain after a significant fall or trauma, especially if you have osteoporosis
These can signal nerve compression that needs timely attention or a non-mechanical cause. They are uncommon — but they’re the reason a clinician always screens for them first.
When Do You Actually Need a Scan?
Most leg pain does not need imaging up front. For typical sciatica or piriformis-type pain without red flags, scans in the first several weeks rarely change what you’d do — which is to manage the symptoms, keep moving within tolerance, and let the nerve settle. Imaging earns its place when red flags appear, when symptoms aren’t improving over roughly six weeks of honest conservative care, or when a decision about injection or surgery is genuinely on the table.
Here’s the part patients find surprising: imaging is great at showing structure and poor at confirming piriformis syndrome. An MRI can reveal a disc herniation pressing a nerve root — useful for true sciatica. But piriformis syndrome is largely a clinical diagnosis, made from history and examination, because the nerve irritation often doesn’t show up clearly on a standard scan. So a “clean” MRI doesn’t rule out piriformis-driven pain, and a “scary” MRI doesn’t prove the disc is your culprit.
If you’ve already had a scan and you’re staring at words like “bulge,” “protrusion,” or “stenosis,” it’s worth understanding how often these findings exist in people without pain — a perspective laid out in this guide on what an MRI finding like stenosis actually means.
Myths Worth Clearing Up
- “Sciatica means a slipped disc.” Not always. The spine is a common source, but the same pain can come from the piriformis, the SI joint, or other deep gluteal structures.
- “If stretching my piriformis doesn’t fix it, nothing will.” If it’s actually spinal in origin, stretching the muscle was never going to be the answer — that’s a diagnostic clue, not a dead end.
- “A bad-looking MRI means I need surgery.” Most nerve-root pain settles without surgery. Imaging findings are one input, not a verdict.
- “Pain down the leg means the nerve is being damaged.” Pain is a protective signal, not proof of damage. Most sciatic-type pain reflects irritation, not injury, and calms down with time and loading.
From the Clinic: Dr. Arora’s Expert Insight
Most people who arrive convinced they have sciatica have never actually had the difference tested — they got the label from a search bar, not from anyone laying hands on the area. That’s not a criticism; it’s just the reality of how these things get named now. The problem is that the label then drives months of the wrong work.
A pattern that comes up repeatedly: someone has been diligently stretching their piriformis for weeks, frustrated that it isn’t helping, when the actual driver is a sensitive nerve root that hates the very forward-bending position many of those stretches put them in. The stretch isn’t neutral — it can mildly aggravate a spinal source while doing nothing for it. The reverse happens too: a true buttock-source pain gets blamed on a disc bulge that showed up on a scan, and the person becomes cautious about bending and lifting when their spine was never the issue.
What gets missed in a quick assessment is provocation testing — does the pain reproduce when we load the spine versus when we tension or compress the piriformis? That single distinction reorganizes the whole plan. Generic advice fails here because it treats “sciatica” as one thing. It isn’t. It’s a symptom with at least two common addresses, and the treatment for one is close to useless for the other. The goal of an early assessment isn’t a fancy scan — it’s figuring out which address your pain is mailing from.
What Can You Do in the First 72 Hours?
In the first 24–72 hours, the aim is to calm the nerve, not to fix it. Avoid the positions that clearly spike your pain, keep gently moving in the range that feels safe, and use short bouts of walking to stop everything from stiffening up. You don’t need to push into pain to “stretch it out,” and you don’t need to lie flat for three days either. Movement in the comfortable middle is the sweet spot.
Practical first steps:
- Reduce sustained sitting. For piriformis-type pain especially, get up every 20–30 minutes. If you must sit, try not to sit on a hard edge or on a wallet in your back pocket.
- Find your easing positions. Most people have one or two positions that genuinely settle the pain. Use them deliberately through the day.
- Walk in small, frequent doses. Even 5–10 minutes a few times a day keeps the nerve gliding and the area from locking up.
- Use heat for muscle-dominant pain. Warmth can help relax a guarding piriformis. For sharp nerve-root pain, do whichever of heat or cold feels better — there’s no universal rule.
- Don’t bedrest. Prolonged rest tends to make sciatic-type pain worse, not better.
🩺 Quick Check: Spine or Buttock?
Answer honestly — yes/no:
- Does your pain start in your lower back before it travels down? (Leans spinal)
- Is the most tender, “press-on-it” spot deep in the middle of your buttock? (Leans piriformis)
- Does coughing or sneezing send a jolt down your leg? (Leans spinal)
- Does pain flare mainly after long sitting and ease once you stand and walk? (Leans piriformis)
- Is there clear numbness or weakness in a specific part of your foot? (Leans spinal — and worth assessing)
More “spinal” answers point toward true sciatica; more “buttock” answers point toward a piriformis source. This is a guide, not a diagnosis — but it tells you which conversation to have with a clinician.
How Does Rehab Progress for Each?
Rehab progresses in phases driven by your nerve’s irritability, not by the calendar. Early on, the job is to settle symptoms and keep moving. As the nerve calms, you load the area progressively — and the direction of loading differs depending on whether the source is your spine or your piriformis. You advance when pain settles and stays settled, not just because a week has passed.
The table below is a general framework. The exercises themselves should be matched to your specific presentation — a point covered well in this overview of how physical therapists structure low back and nerve-pain exercises.
| Phase | Goal | Typical focus | Move on when… |
|---|---|---|---|
| Phase 1 (calm down) | Reduce nerve irritability | Comfortable positions, gentle nerve gliding, short walks, avoiding clear aggravators | Pain is settling and no longer spiking with daily tasks |
| Phase 2 (build tolerance) | Reintroduce load | For spinal: gentle spine-friendly strengthening and hip hinge work. For piriformis: progressive hip rotator and glute strengthening | You can sit, walk, and bend through normal ranges with manageable symptoms |
| Phase 3 (load & restore) | Rebuild capacity | Heavier glute/hip and posterior-chain strengthening, controlled loading patterns | Strength is returning and symptoms stay quiet under load |
| Phase 4 (return to activity) | Resume sport/work fully | Sport- or job-specific demands, running, lifting, longer sitting tolerance | You can meet your real-world demands without flare-ups |
A note on stretching: for piriformis-driven pain, targeted hip-rotator stretching can help once the nerve is calm — but aggressive stretching of an already-irritated nerve often backfires. Strengthening the hip and glutes usually does more lasting work than stretching alone.
Do’s and Don’ts
Do:
- Keep moving in your comfortable range, even on bad days
- Change positions often, especially if sitting is your trigger
- Strengthen your hips and glutes progressively once the acute flare settles
- Track what reliably eases and what reliably aggravates your pain — it’s the best diagnostic data you have
Don’t:
- Aggressively stretch into sharp nerve pain hoping to “release” it
- Sit for hours because resting feels safer — it usually isn’t
- Assume a disc finding on an old scan is the cause of today’s buttock pain
- Chase the piriformis for months if stretching it has never once helped
When Does Conservative Care Fail — and Is Surgery Ever Considered?
Conservative care is considered to have failed when you’ve genuinely committed to it for around 6–12 weeks with no meaningful improvement, or when symptoms are clearly worsening — escalating weakness, spreading numbness, or pain that’s becoming unmanageable despite sensible loading. At that point, further investigation and a specialist opinion make sense. For most people, that crossroad never arrives.
What happens next depends on the source. For true sciatica from a disc or stenosis that hasn’t settled, options may include a nerve-root injection to reduce inflammation, and — in a minority — surgery to decompress the nerve, usually reserved for persistent, significant symptoms or progressive neurological loss. For piriformis syndrome, escalation is more often image-guided injection into or around the muscle; surgery is uncommon and considered only after conservative and injection routes have been exhausted.
The realistic outlook for both is encouraging. The large majority of sciatic-type pain — spinal or piriformis — improves substantially over weeks to a few months with consistent, sensible management. The people who struggle most are usually the ones who either did nothing or did the wrong thing for the wrong source.
🚨 Seek Care Promptly If:
- You develop any numbness in the saddle/groin area or lose bladder or bowel control
- Leg weakness is getting visibly worse week to week (e.g., tripping, foot drop)
- Pain is severe, constant, and unrelieved by any position change
- You have fever, unexplained weight loss, or night pain with your symptoms
These point beyond ordinary mechanical pain and shouldn’t wait out a six-week timeline.
Conclusion
When you strip away the noise, sorting piriformis syndrome vs true sciatica comes down to a simple question asked carefully: is the nerve being irritated at the spine, or deep in the buttock? Spinal sciatica tends to be a line of pain starting at the back, often with numbness or weakness in a specific zone, provoked by bending, coughing, and disc-loading positions. Piriformis-type pain tends to be a tender spot in the mid-buttock, ruled by sitting and hip position, eased by standing and walking.
You don’t need a scan to start, and you usually don’t need surgery to finish. What you need is to identify the right address for your pain so the work you put in actually lands. If the picture is unclear, if red flags appear, or if weeks of honest effort aren’t moving the needle, that’s the moment to get a hands-on assessment rather than guessing.
Frequently Asked Questions
1. Can piriformis syndrome turn into true sciatica?
Not exactly — they’re different sources, not stages of the same thing. Piriformis syndrome already produces sciatic-type pain by irritating the nerve in the buttock; it doesn’t “become” a spinal disc problem. That said, you can have both at once, and ongoing buttock tightness can coexist with a spinal source, which is part of why careful assessment matters.
2. How do I test myself for piriformis syndrome at home?
The most telling home signs are deep mid-buttock tenderness when you press there, pain that flares with prolonged sitting and eases when you stand, and discomfort when you cross the affected leg over the other knee and gently press the knee down. None of these confirm it on their own, but several together point toward a piriformis source rather than a spinal one.
3. Why does my sciatica hurt more when sitting?
Sitting loads things differently depending on the source. With spinal sciatica, rounded sitting increases pressure on the disc and the nerve root. With piriformis syndrome, sitting compresses the muscle directly against the nerve. Either way, getting up regularly and avoiding hard edges or a wallet under one cheek usually helps.
4. Will an MRI tell me which one I have?
An MRI can strongly support a diagnosis of spinal sciatica by showing a disc or stenosis pressing a nerve root, but it’s poor at confirming piriformis syndrome, which is mostly diagnosed clinically. A normal MRI doesn’t rule out a piriformis source, and an abnormal one doesn’t prove the disc is causing your current pain.
5. Is it safe to exercise with sciatic pain?
Generally yes, and movement usually helps more than rest. The key is staying in a range that doesn’t sharply spike your pain and progressing gradually. Avoid pushing hard into nerve pain or aggressively stretching an irritated nerve. If you have red-flag symptoms or clear, worsening weakness, get assessed before continuing.
6. How long does each one take to get better?
Both typically improve substantially over a few weeks to a few months with consistent, sensible management. Piriformis-type pain often responds well once sitting habits and hip strengthening are addressed. Spinal sciatica can take longer if a nerve root is significantly irritated, but most cases still settle without surgery.
7. Could my leg pain be something other than either of these?
Yes. Sciatic-like pain can also come from the SI joint, other deep gluteal structures, hip joint problems, or referred pain — which is exactly why “it’s just sciatica” can be misleading. If your pain doesn’t fit the patterns described here, or isn’t improving, a proper assessment helps rule the alternatives in or out.
Medical Disclaimer
This article is for general educational purposes only and is not a substitute for individualized medical advice, diagnosis, or treatment. Leg and buttock pain can have many causes, some of which require prompt in-person evaluation. Always consult a qualified healthcare professional about your specific symptoms, particularly if you notice any of the red-flag signs described above.
References
- Hopayian K, Danielyan A. Four symptoms define the piriformis syndrome: an updated systematic review of its clinical features. European Journal of Orthopaedic Surgery & Traumatology. 2018;28(2):155–164. doi:10.1007/s00590-017-2031-8
- Park JW, Lee YK, Lee YJ, Shin S, Kang Y, Koo KH. Deep gluteal syndrome as a cause of posterior hip pain and sciatica-like pain. The Bone & Joint Journal. 2020;102-B(5):556–567. doi:10.1302/0301-620X.102B5.BJJ-2019-1212.R1



