“Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.”
You’ve had total knee replacement. The knee is moving — maybe better than it has in years. And yet somewhere in the weeks or months that follow, a new problem emerges: a nagging ache in the lower back, a pull through the hip, or a stiffness through the pelvis that simply wasn’t part of the original complaint.
Your first thought, quite reasonably, is: Did something go wrong?
In the vast majority of cases, nothing went wrong with the surgery. What you are experiencing is a mechanical consequence — a predictable downstream effect of how the knee was functioning before surgery and how the rest of your body has been compensating for it, sometimes for years. Lower back and hip pain after total knee replacement is common, frequently under-discussed in post-operative care, and, for most patients, genuinely resolvable with the right approach.
This guide explains why it happens, how to tell normal compensation from something that needs urgent attention, and what a structured recovery actually looks like.

Key Takeaways
- Lower back and hip pain after total knee replacement most often results from gait compensation patterns, altered lumbopelvic mechanics, and muscular imbalances — not implant failure.
- The knee does not function in isolation. The hip, pelvis, and lumbar spine are direct participants in how the knee loads and moves, both before and after surgery.
- Three factors are consistently overlooked: hip flexor shortening, gluteal deconditioning, and a perceived shift in leg length after deformity correction.
- Imaging is rarely needed for mechanical back or hip pain unless neurological symptoms or specific red flags are present.
- Targeted physical therapy — addressing the kinetic chain above the knee — is the primary and most effective treatment in the vast majority of cases.
- Most patients achieve meaningful improvement within 8–16 weeks of appropriate rehabilitation.
Why Does Your Back and Hip Hurt After Knee Replacement?
Lower back and hip pain after total knee replacement typically develops because the surgery corrects the knee but cannot undo what the rest of the body has learned over months or years of compensating for a painful, stiff, or deformed joint. The hip, pelvis, and lumbar spine adapted to work around the knee — and those adaptations don’t dissolve when the implant goes in. They require deliberate retraining to unwind.
Understanding why this happens requires understanding the knee’s place in the movement chain. The knee sits between two major joints — the hip above and the ankle below. Every load that passes through the lower body passes through the knee; every compensation the knee makes is shared upstream and downstream. The lumbar spine and hip complex are not bystanders in knee disease. They are active participants, and they bear the cost of the knee’s dysfunction long before surgery and well into recovery.
Compensation pattern from pre-operative gait. In the months and often years before total knee replacement, most patients develop what’s called an antalgic gait — a protective walking pattern that minimizes load through the painful knee. This typically involves a shortened stance phase on the affected side, reduced hip extension in the late phase of each step, increased knee flexion, and a subtle lateral trunk shift toward the operated leg. These adaptations are protective and appropriate while the knee is painful. But they reshape muscular function in ways that outlast the knee problem itself.
The gluteal muscles — particularly the gluteus maximus and gluteus medius — progressively underload because the movement patterns that would activate them (hip extension, single-leg stance stability) are being avoided. The hip flexors adaptively shorten from the constant flexed-hip, flexed-knee posture of antalgic walking. The lumbar extensors work harder than they should, stabilizing a pelvis that the hips can no longer control efficiently. This pattern is why so many post-TKR patients report that their back and hip symptoms emerged gradually rather than immediately after surgery — the pain wasn’t caused by the operation; it was uncovered by it.
Perceived leg length discrepancy. Many knees that require replacement have significant structural deformity — most commonly a varus (bow-legged) alignment. Correcting that alignment through surgery mechanically changes the limb’s effective length and geometry. The brain interprets this altered limb geometry as a leg-length discrepancy, tilting the pelvis and loading the lumbar spine asymmetrically. A well-documented consequence of unequal limb loading is increased stress on lumbar motion segments, sacroiliac joints, and the hip on the longer-perceived side. Understanding why post-surgical gait asymmetry can tilt the entire trunk to one side helps explain why many post-TKR patients feel as though their posture has fundamentally shifted after an otherwise successful operation.
Arthrogenic muscle inhibition. Post-operative joint effusion — the swelling that occurs inside the knee after surgery — triggers a neural reflex that inhibits quadriceps activity. This phenomenon, arthrogenic muscle inhibition, means the quad isn’t firing at its normal capacity even when the patient is actively trying to use it. A quad that isn’t contributing its expected share of load forces the hip extensors and lumbar muscles to pick up the difference during activities like climbing stairs, rising from a chair, or walking on inclined surfaces. The lumbar spine is not equipped to absorb this excess demand indefinitely, and over time it registers this as pain.
Underlying spinal pathology newly provoked. A significant proportion of patients undergoing total knee replacement are in their sixties and seventies with pre-existing lumbar disc degeneration or facet joint arthritis that was previously low-level or asymptomatic. Post-TKR, as activity levels gradually increase and gait mechanics shift, these previously quiet structures can become symptomatic. The surgery didn’t cause the lumbar degeneration — it was already there — but the changed movement environment brought it forward.
The relationship between hip mechanics and lumbar loading is explored in more depth here.
What Does the Hip Pain Actually Feel Like, and Where Does It Come From?
Hip pain after total knee replacement typically arises from one of three sources: hip flexor strain at the anterior hip and groin, gluteus medius weakness producing lateral hip pain and unstable walking mechanics, or load redistribution across the pelvis and sacroiliac joints. In a smaller number of cases, increased post-operative activity may bring pre-existing hip osteoarthritis to clinical attention for the first time.
The location of hip pain matters diagnostically. Anterior hip or groin pain — especially pain that appears on first rising from a chair or during the first steps of the day — most often implicates the hip flexor (iliopsoas) complex or the anterior hip joint capsule. These structures are loaded during hip extension, which is precisely the movement that returns as the knee begins to function normally. It’s a painful irony: recovery restores movement that then loads structures that were dormant during the years of antalgic walking.
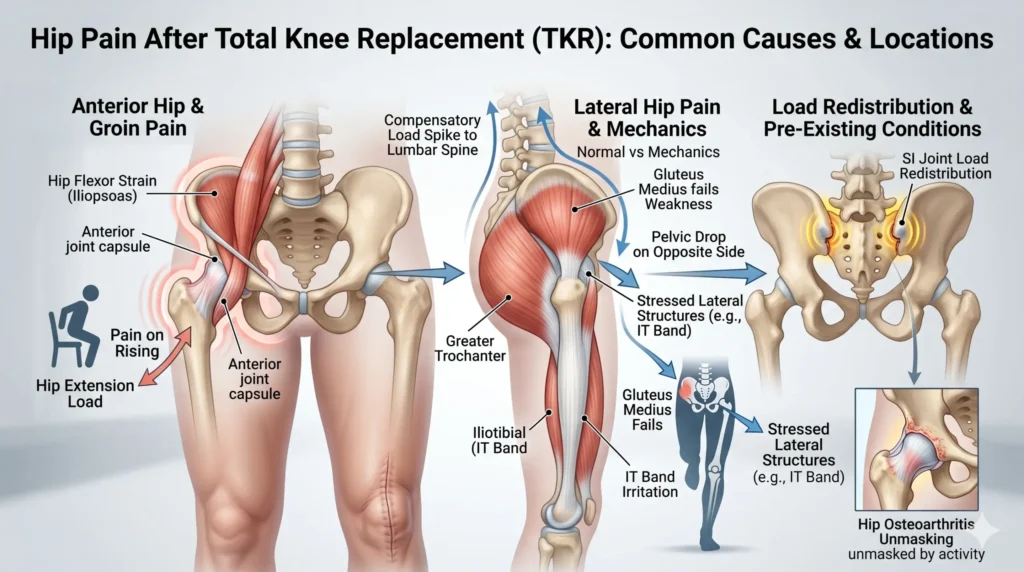
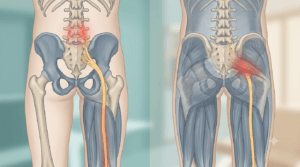
Lateral hip pain, particularly over or around the greater trochanter, more commonly points to gluteus medius weakness or iliotibial band irritation. The gluteus medius is the primary stabilizer of the pelvis during single-leg stance — every step in walking involves a brief moment of single-leg support, and if the gluteus medius on the operated side isn’t working efficiently, the pelvis drops on the opposite side, stressing the lateral hip structures and sending a compensatory load spike into the lumbar spine.
Pain felt deep in the buttock and into the sacroiliac joint area often reflects the asymmetric pelvic torsion that develops when leg loading is unequal — a pattern that, after TKR, is driven by the same perceived leg-length change discussed above.
| Pain Location | Most Likely Source | Aggravating Pattern |
|---|---|---|
| Anterior hip / groin | Hip flexor (iliopsoas) or hip joint | First steps, rising from seated, walking uphill |
| Lateral hip / outer thigh | Gluteus medius weakness, trochanteric bursitis, ITB | Sustained walking, stairs, lying on operated side |
| Buttock / sacroiliac area | Sacroiliac joint dysfunction, piriformis | Prolonged sitting, asymmetric stance, car entry/exit |
| Lumbar, both sides | Lumbar extensor overload | Standing, walking, extension activities |
| Lumbar, one side | SIJ, lumbar facet, or disc | Side-specific loading, twisting, bending |
| Anterior thigh (not hip) | Quadriceps, femoral nerve, implant-adjacent | Direct pressure, resisted knee extension — warrants orthopedic review if localized to implant area |
When Should You Be Worried? Red Flags After Knee Replacement
The large majority of back and hip pain that follows total knee replacement is mechanical and follows a manageable course. However, a small number of presentations suggest pathology that requires prompt attention.
- Calf swelling, warmth, or redness in the operated leg — deep vein thrombosis (DVT) is a recognized complication of joint replacement surgery. A clot that migrates to the lung (pulmonary embolism) is a serious emergency. If this develops, seek same-day assessment.
- Fever combined with joint or back pain — wound infection or deep joint infection can present with pain that appears to come from the back or hip. Do not delay assessment.
- Saddle anesthesia (numbness in the inner thighs and perineum) or any change in bladder or bowel control — this suggests cauda equina involvement, a neurological emergency that requires an emergency department visit.
- Severe, constant night pain that is unrelated to position — especially if accompanied by unexplained weight loss or fatigue; this pattern warrants investigation for non-mechanical pathology.
- New foot drop or rapidly progressing leg weakness — significant motor neurological deficit at the lumbar spine needs prompt assessment.
- Localized knee or thigh ache that appears late in recovery (after an initial period of being pain-free) — this is more specific to the implant than to compensation patterns and warrants orthopedic review.
Does Imaging Actually Help Here?
Imaging after total knee replacement should be guided by clinical findings, not reassurance-seeking. Back and hip pain that varies with position, movement, and load — that gets better with rest and worse with activity — is mechanical in character, and imaging rarely changes management in the early weeks of recovery.
For back pain specifically, ordering a lumbar MRI in the absence of neurological symptoms predictably reveals age-related degenerative changes. These findings are extremely common in the age group undergoing knee replacement, they pre-date the surgery, and they are typically not the cause of the current symptoms. Acting on incidental MRI findings in this context can lead to unnecessary anxiety and interventions that don’t address the real problem.
A patient-focused guide to what back imaging actually shows provides a practical framework for understanding when imaging changes decisions and when it doesn’t.
When imaging is genuinely warranted after TKR:
- Pelvic or hip X-ray — if anterior hip pain is progressive and has a deep groin quality, ruling out advancing hip OA or femoroacetabular pathology is reasonable.
- Weight-bearing knee X-ray — if there is a new or localizing ache in the knee or thigh, alongside or instead of back/hip pain, this checks for implant loosening, subsidence, or periprosthetic fracture.
- Lumbar MRI — reserved for back pain with neurological signs (motor or sensory deficits, bladder or bowel changes) that don’t have an obvious mechanical explanation.
Three Misconceptions That Slow Recovery Down
“The back and hip pain means the implant has failed.” Implant failure has specific presentations: persistent deep knee pain, instability, late-onset swelling, or a thigh ache that was absent in the early post-operative period and has since appeared. New back or hip pain in isolation is almost never implant failure. These are two separate problems with different anatomical sources.
“I should rest until the pain settles before doing exercises.” Sustained rest is counterproductive for muscular compensation pain. The glutes will not recover by being kept still. The hip flexors will tighten further with prolonged sitting. The lumbar stabilizers will decondition. Controlled movement — graded appropriately to current tolerance — is the treatment, not a risk.
“This is just how it is after a big surgery — I have to accept it.” This is the misconception that causes the most avoidable suffering. Post-TKR back and hip pain is not an inevitable permanent trade-off. It has identifiable causes and a well-defined rehabilitation pathway. The overwhelming majority of patients who engage with targeted physical therapy recover well.
From the Clinic: Dr. Arora’s Expert Insight
Most post-operative protocols are appropriately designed around the replaced joint — range of motion targets, quad activation, walking distance. These are important. What they often don’t systematically address is the compensation architecture that the hip, pelvis, and lumbar spine assembled while the knee was deteriorating. That architecture doesn’t dismantle itself just because the knee is now mechanically sound.
What gets missed most reliably is the hip flexor. Not because it’s obscure, but because hip flexor restriction doesn’t announce itself the way quadriceps weakness does. Patients with significant iliopsoas shortening walk with a subtly increased anterior pelvic tilt — more lumbar lordosis than is appropriate, facet joints loaded, gluteal muscles inhibited by that same postural default. These patients don’t describe their hip flexors as the issue; they describe lower back aching after walking fifteen minutes, or a persistent deep groin pull that “just won’t settle.”
The clinical error that comes up repeatedly is trying to load the glutes before restoring hip extension range. Patients are given glute bridges, which is appropriate. But if the hip flexor is still restricting hip extension, the glute bridge gets performed in a limited range, the lumbar spine compensates to fill in the movement the hip can’t supply, and the patient either develops lumbar pain during the exercise or sees minimal glute response. Understanding how gluteal inhibition interacts with lumbar overload is essential for sequencing post-TKR rehab correctly.
The sequence that works clinically: restore hip extension mobility first, then load the glute through the newly available range, then integrate into gait. In that order, not simultaneously, and not in reverse.
What to Do in the Next 72 Hours
If you have lower back or hip pain after total knee replacement right now:
✅ Keep moving — short, frequent walks are preferable to prolonged rest. Stop only if red flags are present (see above).
✅ Break up sitting — after no more than 40–45 minutes in a chair, stand, walk briefly, and change position. Sustained sitting is one of the most reliable aggravators.
✅ Try a gentle supine hip flexor stretch — lying on your back, draw one knee toward your chest while allowing the operated leg to rest flat. Hold 30–45 seconds. This is safe, gentle, and targets the structure that is most commonly overlooked in post-TKR back pain.
✅ Focus on standing tall — most post-TKR patients stand with their hips behind them and their trunk leaning forward. Actively pressing the hips forward into a more upright position offloads the lumbar extensors.
✅ Use ice or heat for local soreness — 10–15 minutes over a cloth; ice for acute soreness, heat for stiffness.
🚨 Seek same-day assessment if: calf swelling or warmth, fever with joint pain, any bladder or bowel change, rapidly worsening weakness in the leg or foot.
Phase-Based Rehabilitation: A Practical Guide
Recovery from post-TKR back and hip pain progresses through stages. Timelines below are approximate — what drives progression is how the body responds, not how many weeks have passed.
| Phase | Approx. Timeline | Primary Goal | Key Exercises | Progression Criteria |
|---|---|---|---|---|
| 1 — Normalise | Weeks 1–6 post-TKR | Reduce pain, restore basic hip extension range, begin deliberate gait retraining | Supine hip flexor stretch, heel slides, short arc quads, standing hip extension (wall support), deliberate heel-to-toe walking pattern | Pain ≤ 4/10 during activity; can stand 20+ minutes without significant back pain increase |
| 2 — Rebuild | Weeks 6–14 | Restore gluteal strength, address hip-lumbar coordination, normalize gait symmetry | Double-leg glute bridge, side-lying hip abduction, clamshells, supported single-leg stance (10–15 sec), step-ups on a low platform (15–20 cm / 6–8 in) | Can walk 20+ minutes without a visible limp; glute bridge held 30 seconds without lumbar substitution |
| 3 — Integrate | Weeks 12–20+ | Full kinetic chain loading, return to community walking, stairs, ADLs | Single-leg glute bridge (progressive), lateral resistance band walks, controlled hip hinge, stair negotiation with full control, varied terrain walking | Symmetric gait on video observation; 45+ minutes of continuous walking tolerated; back and hip pain ≤ 2/10 at rest |
Do’s and Don’ts
Do:
- Walk regularly — even if the back or hip is sore, provided pain stays below 5/10 and doesn’t escalate significantly afterward
- Stretch the hip flexors daily — this is consistently the most neglected element of post-TKR kinetic chain recovery
- Sleep with a pillow between your knees if side-lying — this reduces rotational stress on the lumbar spine and hip simultaneously
- Pay deliberate attention to your walking pattern — push through the operated leg, allow the hip to extend behind you, and avoid the shortened shuffle that pre-operative pain established
- Report persistent or worsening symptoms to your physical therapist or surgeon — linear improvement is expected; plateaus or regressions need explanation
Don’t:
- Avoid movement because it might make things worse — sustained rest actively delays the muscular retraining that resolves these symptoms
- Rely on isolated core exercises as the primary intervention — targeting the trunk in isolation without addressing hip mobility and glute function is a common reason rehab stalls in post-TKR patients
- Sit for more than 45–50 minutes without a movement break — sustained hip flexion at this stage is a direct antagonist to recovery
- Assume worsening back pain is always implant-related — the clinical picture matters; localization, timing, and character determine whether orthopedic review is indicated
- Self-treat the lumbar spine in isolation — treating the back as the primary problem, when it is the compensation site, misses the driver
Return to Activity: What’s Realistic
For most patients, meaningful improvement in lower back and hip pain after total knee replacement is achievable within 8–16 weeks of consistent, targeted rehabilitation. Full activity recovery — comfortable walking, managing stairs, driving, and light exercise — typically comes together in the 3–5 month window post-surgery.
For those returning to specific activities:
Driving usually becomes comfortable once hip flexor mobility and gluteal strength improve enough to support prolonged seated hip flexion followed by smooth transition to standing. For most patients this aligns with the 6–10 week post-operative window, though individual variation is significant.
Cycling (stationary initially) is often well tolerated earlier than most patients expect, and is particularly useful because the pedaling motion directly trains the hip extension pattern that transfers to improved gait mechanics.
Prolonged standing or walking — whether at work, travelling, or recreating — depends most heavily on gluteal endurance. This is typically the last functional capacity to fully restore, and its return is one of the most reliable indicators that the kinetic chain rehab has been effective.
A structured approach to physical therapy exercises for lower back pain offers additional guidance for the lumbar component of recovery alongside knee-focused rehabilitation.
When Conservative Care Isn’t Enough
Physical therapy and graded exercise resolve back and hip pain after total knee replacement in the large majority of cases. If pain is not meaningfully improving after 12 weeks of appropriate, well-supervised rehabilitation — or if it is actively worsening — a more comprehensive review is warranted.
Consider referral for further assessment if:
- Neurological symptoms (weakness, sensory change, bladder or bowel changes) develop at any point
- A late-onset thigh or knee ache appears after an initially pain-free period — this is more specifically related to the implant and needs orthopedic evaluation
- Hip pain is anterior, progressive, and accompanied by a mechanical click or catching — this may indicate advancing hip OA that now requires its own management pathway
- Pain is severe, constant, and non-mechanical despite 12+ weeks of appropriate care
Surgery is rarely indicated for post-TKR back or hip pain. The specific scenarios where secondary surgical intervention becomes relevant are implant failure (confirmed loosening, deep infection, periprosthetic fracture, or instability), progressive hip OA that has crossed the threshold for joint replacement, or confirmed lumbar nerve root compression causing motor deficits that have failed a full course of conservative management. These are clinical decisions made on the basis of imaging, functional decline, and thorough assessment — not on the basis of pain alone.
Prognosis: What to Reasonably Expect
Lower back and hip pain after a successful total knee replacement can be demoralising, particularly when the knee itself is recovering well. The reassuring reality is that these symptoms are predominantly mechanical in origin, predictable in their drivers, and highly responsive to targeted rehabilitation.
The compensation patterns that took months or years to develop don’t resolve in a few sessions of exercise. Restoring normal hip extension mobility, reactivating the gluteal complex, retraining gait mechanics, and progressively reloading the kinetic chain above the knee is a process that unfolds over weeks. For most patients, that process leads to a meaningful and lasting outcome.
Conclusion
Lower back and hip pain after total knee replacement reflects the body’s upstream response to years of knee dysfunction — and the mechanical readjustment required when that dysfunction is surgically corrected. It is not, in the vast majority of presentations, a sign of implant failure, permanent nerve injury, or surgical error.
The effective treatment path focuses on what the operation couldn’t address: hip flexor mobility, gluteal strength, lumbopelvic stability, and the restoration of a walking pattern that no longer needs to work around a damaged knee. With a rehabilitation program that looks above the knee — not just at it — most patients managing lower back and hip pain after total knee replacement recover well and return to the activities that the surgery was originally meant to restore.
If symptoms are worsening, progressing neurologically, or failing to improve after 8–12 weeks of appropriate physical therapy, a formal clinical assessment is the right and timely next step.
Frequently Asked Questions
Is it normal to have back pain after total knee replacement? Yes — it is a recognized and common occurrence. Back pain after total knee replacement typically develops from gait compensation patterns, altered leg loading, and muscular imbalances above the knee rather than from any problem with the implant itself. For most patients, it responds well to targeted physical therapy.
How long does hip pain last after knee replacement? Hip pain that develops as a result of gait compensation and muscular imbalance after total knee replacement generally improves meaningfully within 8–16 weeks of targeted rehabilitation. The exact duration depends on how established the pre-operative compensation patterns were, how consistently rehab is engaged with, and whether there are any additional contributing factors such as hip OA. Hip pain that is progressive, anterior in location, and not improving at 12 weeks warrants assessment to rule out hip joint involvement.
Can knee replacement surgery cause sciatica? True sciatica — pain from compression or irritation of the sciatic nerve originating in the lumbar spine — is not directly caused by the knee replacement procedure. However, post-TKR gait changes and lumbar muscular overload can provoke or worsen symptoms in patients who have pre-existing lumbar disc or nerve pathology. If leg pain has a clear dermatomal quality (following the path of the sciatic nerve down the back of the leg into the foot), a lumbar assessment is warranted.
Will the back and hip pain go away on its own? It may improve gradually as gait mechanics normalize post-surgery, but waiting passively tends to be a slower route than targeted rehabilitation. The hip flexor shortening and gluteal deconditioning that drive most post-TKR back and hip pain require active correction. Patients who engage with structured physical therapy consistently do better than those who rest and wait.
What exercises help lower back pain after knee replacement? The most effective early exercises target hip extension mobility and gluteal activation: supine hip flexor stretching, standing hip extension with wall support, double-leg glute bridges, and side-lying hip abduction. These address the specific muscular imbalances that drive lumbar overload in this population. Isolated lumbar exercises — abdominal crunches, lumbar rotation — are generally of limited value if the hip mobility deficit is not addressed first.
When should I be worried about back pain after knee replacement? Seek prompt assessment for: calf swelling or warmth (possible DVT), fever with joint or back pain, any change in bladder or bowel function, saddle-area numbness, new foot drop or rapidly progressing leg weakness, or severe constant night pain that is not position-dependent. These presentations are uncommon, but they require timely evaluation and should not be observed at home.
Does total knee replacement affect the hips? Yes — indirectly but significantly. Total knee replacement changes how load is distributed through the entire lower limb, alters gait mechanics, and corrects deformities that may shift the effective limb length. All of these changes directly influence how the hip joint is loaded during walking and daily activity. Pre-existing hip conditions may become symptomatic for the first time, and the hip musculature frequently requires deliberate retraining as part of post-TKR rehabilitation.
Can a perceived leg length change from knee replacement cause lower back pain? Yes. Correcting a significant varus or valgus deformity through total knee replacement changes the effective geometry of the limb, which the brain can interpret as a leg-length discrepancy. This perceived asymmetry causes compensatory pelvic tilting that loads the lumbar spine and sacroiliac joint unequally. The association between lower limb length asymmetry and lumbar spine stress is well established and is one of the recognized contributors to post-TKR back pain.
Medical Disclaimer
This article is written for educational purposes and reflects general clinical knowledge in musculoskeletal physiotherapy and rehabilitation. It is not a substitute for professional medical advice, diagnosis, or treatment. Individual presentations vary, and what is appropriate for one patient may not be appropriate for another. If you are experiencing back or hip pain after total knee replacement, consult your surgeon, physiotherapist, or healthcare provider for an assessment tailored to your specific situation. Do not ignore or delay seeking professional care because of information in this article.
References
- Ziętek P, et al. “The Temporal–Spatial Parameters of Gait After Total Knee Arthroplasty.” Journal of Clinical Medicine. 2025;14(13):4548. DOI: 10.3390/jcm14134548. Published June 26, 2025.
- Golightly YM, et al. “Leg length discrepancy and osteoarthritis in the knee, hip and lumbar spine.” Journal of Rheumatology. 2015;42(11):2116–22. PMID: 26500356.