“Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.”
If you live with ankylosing spondylitis, you already know the cruel arithmetic of the night. You are exhausted, you finally lie down, and within a few hours the very stillness that is supposed to restore you starts to stiffen your spine and wake you. By 4 a.m. you are pacing the bedroom, not because you want to, but because moving is the only thing that takes the edge off. That second-half-of-the-night ache is not in your head, and it is not weakness. It is the signature of inflammatory back pain, and it behaves almost backwards compared with an ordinary “bad back.”
This guide is about working with that biology instead of fighting it: which positions tend to help, how to build a pillow setup that supports a spine that may be losing some of its natural curves, and the night-time habits that take the sting out of the early-morning stiffness storm. Positioning will not switch off the disease, but for many people it is the difference between a fragmented night and a tolerable one.

Key Takeaways
- Ankylosing spondylitis pain is inflammatory, meaning it tends to worsen with prolonged rest and ease with movement — the opposite of most mechanical back pain.
- Back-lying (supine) with a thinner pillow is usually the most spine-friendly default, because it discourages the forward-curled posture the disease already pushes you toward.
- Pillow height matters more than people think — a tall stack quietly drives the neck and upper back into flexion over years.
- Waking in the second half of the night with stiffness that improves once you get up and move is a classic pattern, not a sign you chose the “wrong” position.
- A sudden, new, severe spinal pain after even a minor knock deserves urgent assessment — a long-standing fused spine can fracture more easily than people expect.
- Sleep setup is a powerful adjunct, but consistent exercise and proper medical disease control remain the foundation of care.
Why does ankylosing spondylitis make sleep so difficult?
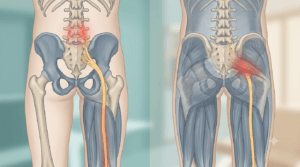
Ankylosing spondylitis is a chronic inflammatory arthritis that mainly targets the spine and the sacroiliac joints, where the base of the spine meets the pelvis. Because the inflammation is driven by an active immune process rather than by a one-off mechanical injury, the pain follows a rhythm: it tends to quiet down when you are active during the day and flare when you hold still for a long stretch — which is exactly what sleep asks you to do. This is why so many people describe their worst hours as the early morning.
There is a simple biological reason behind the dawn stiffness. When inflamed tissue stays motionless for hours, inflammatory fluid and chemical mediators are thought to pool and settle around the joints, a sticky, “gelled” state that movement then disperses. Clinicians sometimes call this the gel phenomenon. Add to that the slow structural changes of the disease — inflammation at the entheses (where ligaments and tendons anchor to bone), gradual loss of the lower back’s natural inward curve, and in some people a creeping forward bend of the upper spine — and you have a body that is both irritable and increasingly shaped against comfortable lying.
The chest can join in too. Ankylosing spondylitis can stiffen the small joints where the ribs meet the spine, so some people notice that lying in certain positions makes a full, easy breath harder to take. None of this means the night is hopeless. It means the goal is not to lie perfectly still in the ideal position — it is to keep the spine in a friendly shape, reduce the overnight stiffening, and make it easy to move when you need to.
What is the best sleeping position for ankylosing spondylitis?
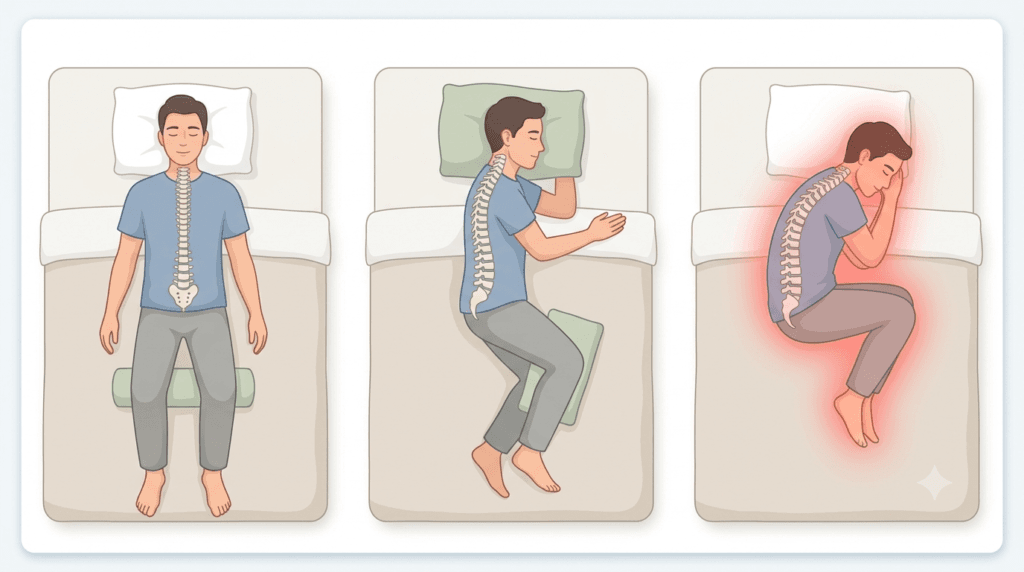
For most people with ankylosing spondylitis, sleeping on your back on a supportive, medium-firm surface is the most spine-friendly default, because it keeps the spine relatively straight and lengthened and resists the forward-curled posture the disease already encourages. Side-sleeping is perfectly acceptable if you stay long rather than curling tightly. The position to be wary of long-term is anything that locks you into a deep, sustained flexed-forward shape.
Here is the reasoning behind each option, because the “why” is what lets you adapt it to your own body.
Back (supine) — the usual first choice. Lying flat keeps the spine close to neutral and gently discourages the forward bend that ankylosing spondylitis tends to drive over years. Keep the head pillow on the lower side so your chin is not tipped toward your chest all night. If the lower back’s natural curve has flattened and the small of your back feels unsupported, a slim rolled towel or low lumbar pillow under it can restore a little arch.
Side — fine if you stay long. A relaxed side-lying position is comfortable for many people, but the trap is the fetal curl: knees tucked high, back rounded, chin down. Held for hours, that posture quietly reinforces exactly the spinal shape you are trying to avoid. The fix is small — keep your hips and knees only gently bent, and place a pillow between your knees (roughly the width of your hips, so the top leg does not drag your pelvis into a twist).
Front (prone) — useful in short doses, not all night. Brief spells lying face-down were traditionally encouraged in ankylosing spondylitis precisely because they push the spine into extension, the opposite direction to the disease’s forward pull. The problem is the neck, which has to crank to one side to let you breathe. Treat prone lying as a few-minute daytime or pre-sleep extension stretch rather than a sleeping position.
| Position | Why it can help in AS | The catch to avoid |
|---|---|---|
| Back (supine) | Keeps spine long and neutral; resists forward flexion | A tall pillow tipping the head forward |
| Side (long) | Comfortable; easy to settle into | Curling tightly into a flexed, fetal shape |
| Front (prone), brief | Extends the spine against the disease’s forward pull | Sustained neck rotation; not for full nights |
| Recliner / propped half-sitting | Tempting during a flare | Long-term hip and spine flexion if it becomes the norm |
How should you set up pillows for ankylosing spondylitis?
The guiding principle is simple: pillows should fill the gaps your spine cannot, without pushing any part of you into a curled or tipped position. A neck pillow should be just tall enough to keep your head level — neither tilted forward nor dropped back — and side- or back-sleepers add a knee or lumbar pillow only where there is an actual unsupported space.
Walk it through, top to bottom:
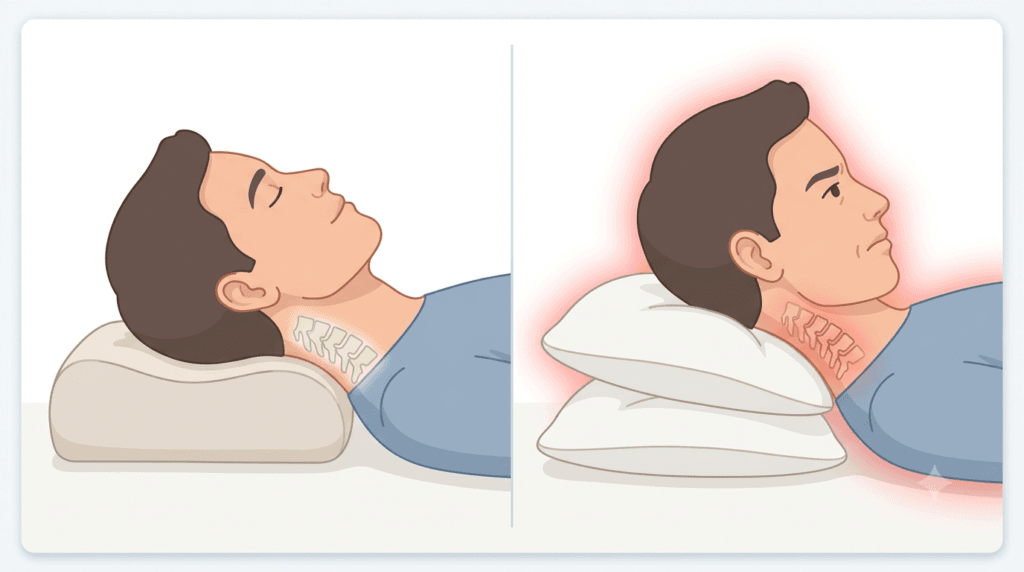
- Head and neck. Aim for a pillow that keeps your nose roughly in line with your breastbone when you are on your back, and that fills the gap between your ear and the mattress when you are on your side — no more. A contour or adjustable pillow earns its place here because a fused or stiffening neck does not forgive a pillow that is too high. If your upper back has begun to round, you may feel like you need a taller pillow just to see the room; resist stacking, because that height is doing the disease’s work for it.
- Lower back. If your lumbar curve has flattened, a low roll (a folded towel works) under the small of the back while supine can take the “floating” pressure off and let the muscles settle.
- Between or under the knees. Side-sleepers: a pillow between the knees keeps the pelvis level. Back-sleepers who feel pulling in the low back can try a slim pillow under the knees — but keep it modest, since a large bolster there encourages hip flexion, another forward-curl input you do not want night after night.
For an inflammatory spine, heat is one of the most reliable comforts there is — a warm shower before bed loosens the morning-style stiffness, which is the same reasoning behind choosing heat over ice for this kind of stiff, non-acute back pain.
How is this different from ordinary mechanical back pain?
The fastest way to tell inflammatory back pain from a common mechanical strain is the pattern over a night and a morning: inflammatory pain is worse after rest, drags on with stiffness for more than half an hour after waking, and improves with movement, whereas mechanical pain typically eases with rest and worsens when you load or move the back. That single distinction reshapes the whole sleep strategy.
| Feature | Inflammatory pattern (AS-type) | Mechanical pattern |
|---|---|---|
| When it’s worst | Second half of night, early morning | After activity or specific movements |
| Morning stiffness | Often more than 30–60 minutes | Brief, usually under a few minutes |
| Effect of rest | Worsens it | Tends to relieve it |
| Effect of movement | Eases it | Can aggravate it |
| Typical age of onset | Usually before 40–45 | Any age |
| Response to lying still | Stiffens and wakes you | Often soothing |
This is also why generic “rest your back” advice misfires here, and why a position that feels great for someone whose pain comes on after bending or lifting may do nothing for an inflammatory spine. The mechanisms are different, so the night-time playbook has to be different.
From the Clinic: Dr. Arora’s Expert Insight
Ask ten people with ankylosing spondylitis what their physiotherapist told them, and a surprising number will say some version of “find a comfortable position and try to stay in it.” I understand the instinct, but for this condition it is close to backwards. A pattern that comes up again and again is the person who has spent months chasing the perfect mattress and the perfect pillow, convinced that the right setup will finally let them sleep through — and they are quietly devastated when it does not, because they assume they have failed at the one thing they could control.
What often gets missed is that the night-waking is frequently the inflammation talking, not the bedding. The most useful reframe I can offer is permission to move at 4 a.m. instead of lying there grimly trying to outlast the stiffness. Getting up, walking the hallway, doing two or three gentle extension movements, and then going back down often resets the next stretch of sleep far better than white-knuckling it. The position and pillows are there to keep the spine in a kind shape and make that getting-up easy — they are scaffolding, not a cure.
The other thing I find myself repeating: the bed is downstream of the day. People who keep their spine mobile with regular, slightly uncomfortable movement during the day almost always report easier nights than people who protect their backs into rigidity. Generic advice fails here because it treats an inflammatory disease like a pulled muscle. They are not the same animal, and the sleep strategy has to respect that.
When should night pain make you worried?
Most night-time ankylosing spondylitis pain, however miserable, is the familiar inflammatory ache and not an emergency. The signals that warrant prompt assessment are a sudden change from your usual pattern — new, severe, localized spinal pain (especially after even a minor fall or knock), new numbness, weakness, or tingling in the limbs, any loss of bladder or bowel control, or systemic signs like unexplained fever or weight loss.
A point that is specific to a long-standing, partly fused spine deserves emphasis: a spine that has stiffened and fused over years can also become more brittle, so an impact that would barely bruise someone else can crack it. New, sharp, unrelenting pain after a seemingly trivial bump is a reason to be checked, not to wait and see. Separately, ankylosing spondylitis can flare the eye — sudden eye pain, redness, light sensitivity, or blurred vision (a possible uveitis) is its own urgent issue and should be seen quickly.
⚠️ Seek care promptly if you notice:
- Sudden, severe new back or neck pain, particularly after a minor fall or impact
- New weakness, numbness, or pins-and-needles in the arms or legs
- Any change in bladder or bowel control
- A red, painful, light-sensitive eye or sudden blurred vision
- Fever, night sweats, or unexplained weight loss alongside the pain
These point beyond routine stiffness and deserve same-day or urgent evaluation.
When is imaging actually needed?
Imaging does not pick your pillow, and you do not need a scan to justify changing how you sleep. Imaging earns its place when it would change the plan — confirming the diagnosis, gauging how active or advanced the disease is, or investigating a sudden, severe new pain that could signal a fracture. For routine night stiffness that follows your usual pattern, repeat scans rarely add anything.
In practice, an MRI of the sacroiliac joints and spine is the tool that shows active inflammation, which is what matters early or when treatment decisions hang in the balance. Plain X-rays show the slower, structural story — joint changes and fusion that build over years. The one scenario where imaging shifts from “elective” to “do not delay” is that sudden severe pain after trauma in a spine that has been fusing, where ruling out a fracture is the priority.
Practical management: building a night that works
What to do in the next few nights
You do not have to overhaul everything at once. Layer these in over a few evenings and notice what your body says.
- Warm up before bed. A warm shower or a few minutes with a heat pack loosens the inflammatory stiffness so you start the night less rigid.
- Move before you settle. Two or three gentle spinal extension and rotation movements signal the system that the day is not over yet and take some of the gel out of the joints.
- Set the pillow low. Start one notch lower than feels natural, especially on your back, and let your neck stay long rather than tipped forward.
- Default to your back, stay long on your side. Avoid the tight fetal curl; use a knee pillow if you side-sleep.
- Give yourself permission to get up. If you wake stiff in the early hours, get up, walk and move gently for a few minutes, then return. This is a feature of the disease, not a failure of your setup.
How to think about progression
Sleep improvement in ankylosing spondylitis is rarely linear, and it tracks your overall disease activity more than any single gadget. A reasonable way to read your own progress:
| Phase | What it looks like | What to focus on |
|---|---|---|
| Settling a flare | Frequent waking, long morning stiffness | Heat, easy movement, position basics, medical review of disease control |
| Stabilizing | Waking less, stiffness shortening | Consistent daytime mobility, refining pillow height |
| Maintaining | Mostly tolerable nights | Keeping the exercise habit that earned the better sleep |
The thread running through every phase is movement. Major international rheumatology guidance places non-pharmacological care — patient education and regular exercise — as a cornerstone of managing axial spondyloarthritis, sitting alongside medication rather than behind it, as set out in the 2022 ASAS-EULAR recommendations. Your bedroom setup supports that work; it does not replace it.
Do’s and don’ts specific to AS
Do:
- Keep daytime mobility up, even when stiff — a mobile spine sleeps better than a guarded one.
- Use heat before bed as a deliberate stiffness-reducer.
- Re-check your pillow height every several months as your posture changes.
Don’t:
- Don’t sleep long-term in a recliner or heavily propped-up; the hip-and-spine flexion adds up.
- Don’t stack pillows to “see better” if your upper back is rounding — that height feeds the curve.
- Don’t equate a sleepless night with a personal failure; treat it as information about disease activity.
When the basics aren’t enough
If your nights stay broken despite a sensible setup, consistent exercise, and good positioning, that is usually a message about disease control, not bedding. Persistent night pain and long morning stiffness are among the things rheumatologists use to judge whether current treatment is doing its job, and they may prompt a change in medical management. Sleep, here, is a useful barometer — when it stays poor, it is worth a conversation about whether the underlying inflammation is adequately controlled, not just another mattress. Prolonged static postures during the day, such as a long stiff commute, can compound it, which is why people often notice the link between long spells of sitting and a worse back.
Conclusion
Sleeping well with ankylosing spondylitis is less about discovering one magic position and more about respecting the disease’s logic: keep the spine in a long, friendly shape, keep pillows low and supportive, warm up before bed, and give yourself full permission to get up and move when the early-morning stiffness arrives. The reason “how to sleep with ankylosing spondylitis” has no single tidy answer is that the night is downstream of your daytime movement and your overall disease control — fix those, and the bed becomes a far kinder place. Start with the back-sleeping, low-pillow default tonight, and adjust from there.
Frequently Asked Questions
1. What is the single best sleeping position for ankylosing spondylitis?
For most people, lying on your back on a supportive, medium-firm surface with a lower pillow is the best default, because it keeps the spine long and resists the forward-curled posture the disease promotes. Long side-lying with a knee pillow is a reasonable alternative if back-sleeping is uncomfortable.
2. Why does my back hurt more at night than during the day?
Ankylosing spondylitis pain is inflammatory, so it tends to worsen with the prolonged stillness of sleep and ease with movement — the reverse of a typical muscle strain. Inflammatory fluid is thought to settle around the joints overnight, producing the early-morning stiffness that movement then clears.
3. Should I sleep on a firm board or a very hard mattress?
No — a rock-hard surface is not the goal. A supportive, medium-firm mattress that keeps the spine level without sagging is generally more comfortable and more sustainable than an extremely hard one, which can create pressure points without offering any extra benefit.
4. Is it bad that I wake up and have to walk around at night?
Not at all — it is a classic feature of inflammatory back pain. Getting up to move and gently stretch often resets your sleep better than lying still and waiting the stiffness out, so treat it as part of managing the condition rather than a sign you have done something wrong.
5. Can the right pillow stop my neck from stiffening?
A well-chosen pillow will not prevent the underlying disease, but a pillow that is too tall can quietly worsen a forward-tipped neck posture over time. Keeping the head level — neither pushed forward nor dropped back — protects comfort and discourages that drift, which matters if the neck is already stiffening.
6. Will fixing my sleep position cure my ankylosing spondylitis pain?
No. Positioning is a genuinely helpful adjunct, but it does not control the inflammation. Regular exercise and appropriate medical treatment remain the foundation; if nights stay broken despite good positioning, that usually points to disease activity that needs a medical review rather than another change of bedding.
7. When should night pain send me to a doctor urgently?
Seek prompt care for sudden severe new spinal pain (especially after a minor fall), new limb weakness or numbness, loss of bladder or bowel control, a red painful light-sensitive eye, or fever and weight loss. A spine that has fused over years can fracture more easily, so a new sharp pain after a minor knock should not be ignored.
Medical Disclaimer
This article is for general education and is not a substitute for individual medical advice, diagnosis, or treatment. Ankylosing spondylitis varies considerably from person to person, and sleep strategies that suit one individual may not suit another. Always consult a qualified rheumatologist, physician, or physical therapist about your own symptoms and before making changes to your management — particularly if you have new, severe, or rapidly changing symptoms.
References
- Ramiro S, Nikiphorou E, Sepriano A, et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Annals of the Rheumatic Diseases. 2023;82(1):19–34. doi:10.1136/ard-2022-223296. https://doi.org/10.1136/ard-2022-223296