“Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.”
A disc herniation at L5-S1 hits powerlifters in a way it does not quite hit anyone else. The movement patterns at the center of the sport — the deadlift, the squat, the specific bracing and loading demands of competition — are also the patterns most directly affected by this injury. So when the diagnosis arrives, the fear that follows is not just about pain. It is about whether the sport continues.
L5-S1 herniation recovery for powerlifters is a specific clinical challenge, not a variation on generic back pain management. It requires a protocol that accounts for barbell loading patterns, intra-abdominal pressure dynamics, hip hinge mechanics, and the demands of competitive return. General advice — rest, gentle movement, time — is not wrong for powerlifters. It is just not nearly enough.
The short answer to the core fear: most powerlifters recover. Most return to training. Many compete again. The timeline is longer than you want it to be, and the path is more structured than most people expect. This article explains how it works, from the first painful week through return to the platform.

Key Takeaways
- L5-S1 is the most heavily loaded disc in the lumbar spine. Powerlifting places specific compressive and shear forces on this segment through the squat, deadlift, and bracing mechanics.
- Nerve root irritation — not the size of the herniation on imaging — drives most symptoms. Leg pain distribution and neurological changes are the most clinically useful signals.
- Conservative management recovers the majority of athletes, including those with significant herniation and radiculopathy.
- A phase-based rehab protocol — not unstructured rest — is what drives recovery in load athletes.
- Recognizing the one genuine emergency in disc herniation (cauda equina syndrome) is the most important clinical judgment call in this condition.
What Actually Happens to the L5-S1 Disc During Heavy Lifting?
The L5-S1 disc sits at the base of the lumbar spine, between the fifth lumbar vertebra and the sacrum. It is the most heavily loaded segment in the spine, and the one that generates more herniations than any other level. Under heavy compound loading, a combination of axial compression and posterior shear stress can push the soft inner disc material through a weakened section of the outer ring, producing a herniation. Understanding this mechanism — not just the anatomical label — matters for making sense of what recovery actually demands.
The disc has two functional layers. The nucleus pulposus is the gel-like inner core, kept under constant hydrostatic pressure. The annulus fibrosus is the fibrous outer ring that contains it. Herniation occurs when the nucleus pushes through a weakened or torn area of the annulus — typically at the posterior-lateral wall, where the annulus is thinnest and where rotational and shear stresses concentrate during spinal flexion under load. The term “slipped disc” is anatomically wrong: nothing slips. The nucleus migrates through the annulus.
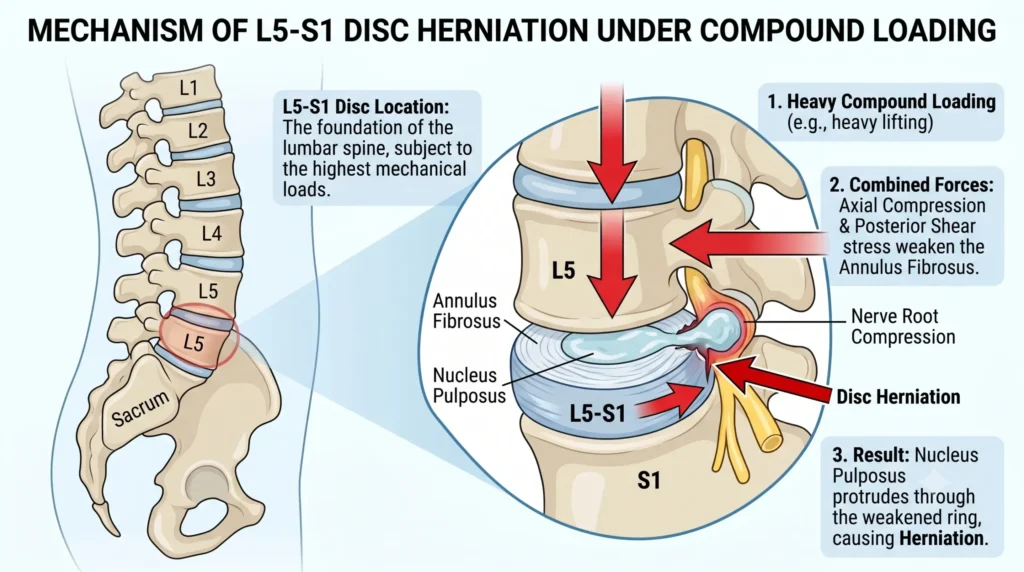
At L5-S1, the geometry creates specific vulnerability. The lumbosacral junction is a transition zone where spinal mobility meets pelvic rigidity, producing high shear forces during end-range loading. A conventional deadlift at the base of the pull, a heavy squat at full depth, or inadequate bracing at any phase of the competition lifts all concentrate mechanical stress at this segment. In competitive powerlifters, disc wall integrity accumulates microdamage over years — which means a single high-effort session can be the one that produces a clinical herniation rather than a purely subclinical event.
The nerve implications depend on the direction of the herniation. Posterior-lateral migration typically contacts the S1 nerve root, producing symptoms into the posterior calf, outer foot, and toe flexors. Central or intraforaminal herniation may involve the L5 root, with symptoms along the lateral shin and dorsum of the foot. These are patterns, not rules — mixed presentations are common — but the distinction guides assessment and helps track whether recovery is progressing in the right direction.
How Do You Know It’s a Disc Herniation — and Not Something Else?
An L5-S1 disc herniation typically produces a combination of lower back pain and leg symptoms — pain, numbness, tingling, or weakness — that follow a nerve root distribution into the buttock, posterior thigh, calf, or foot. What separates it from other common sources of low back and leg pain is the neurological character of those leg symptoms and specific aggravating factors that increase intra-abdominal pressure, such as coughing, sneezing, or straining.
The differential diagnosis matters, because several conditions overlap in presentation and each has different recovery logic.
| Presentation | Likely Structure | Key Distinguishing Feature |
|---|---|---|
| Unilateral low back ache, worse with extension, no leg symptoms | Facet joint irritation | Eased by flexion; no radicular pattern; no neurological signs |
| Buttock and posterior hip pain, worsens with sustained sitting | Piriformis / deep gluteal referral | Local tenderness on pressure; passive hip rotation reproduces pain |
| Groin or anterior thigh pain, restricted hip rotation | Hip joint pathology | Hip range of motion actively and passively limited; no neurological signs |
| Back pain worse at rest or night, constitutional symptoms | Non-mechanical cause | Night symptoms, fever, unintentional weight loss, history of malignancy — seek urgent assessment |
| Posterior leg pain, altered sensation, worsened by cough or sneeze | L5 or S1 nerve root involvement | Neurological distribution matches dermatomal territory; neural tension signs present |
The L5 versus S1 distinction: L5 nerve root involvement produces symptoms along the outer shin and into the top of the foot, with potential weakness of big-toe extension. S1 involvement follows the posterior calf and outer sole of the foot; weakness of plantarflexion — difficulty standing fully on tiptoes on the affected side — is a useful functional indicator. Tracing the dominant symptom pattern guides assessment and provides a useful benchmark for monitoring recovery progress over weeks.
When Is This a Medical Emergency?
The vast majority of L5-S1 disc herniations are not emergencies. One specific complication is. Cauda equina syndrome — compression of the nerve bundle at the base of the spinal canal that controls the lower limbs, bladder, and bowel — requires emergency surgical decompression. Missing the intervention window has consequences that are not recoverable with conservative care.
Seek emergency care without delay if any of the following develop:
- Inability to urinate, or new urinary incontinence
- Bowel incontinence or sudden loss of bowel control
- Numbness or tingling in the saddle region (inner thighs, perineum, or genitalia)
- Rapidly progressive weakness in both legs simultaneously
- Loss of deep tendon reflexes bilaterally
These symptoms indicate herniated disc material has migrated into the central canal in sufficient volume to compress multiple nerve roots at once. This is a surgical emergency, not a physiotherapy presentation. Time from symptom onset to decompression directly affects outcome.
Outside of cauda equina, seek prompt assessment within days — not weeks — if neurological deficits are worsening rapidly rather than fluctuating, or if you have unexplained night sweats, fever, or significant unintentional weight loss alongside back pain, or a personal history of cancer.
Does an MRI Actually Change Anything at L5-S1?
For most presentations in the acute phase, it does not change management. MRI confirms the presence, location, and approximate size of a herniation and helps rule out fracture, infection, and malignancy — but it cannot tell you how much pain the herniation is producing, and it does not predict recovery trajectory. This is the most important and most consistently misunderstood point about imaging in disc herniation.
Population-based imaging studies have found herniations, bulges, and disc degeneration on MRI in people with no back pain at all. A large-appearing herniation on imaging is not a large-pain prognosis. The clinical picture — nerve function, symptom behavior, centralization pattern, response to position changes — is far more useful for predicting recovery than the radiological report.
When imaging is clinically appropriate:
- Neurological signs (weakness, reflex asymmetry, sensory deficit) are present and worsening
- Red flag symptoms suggest a non-mechanical or urgent cause
- Conservative management over 6–12 weeks has not produced meaningful functional improvement
- Surgical consultation is being actively considered and anatomical detail is needed
When imaging can safely wait:
- Local back pain only, no neurological signs, symptoms are improving
- The clinical goal is reassurance rather than directing a treatment change
A finding that frequently appears alongside herniation in powerlifters is Modic signal change at the vertebral endplates — a different structural process, with its own clinical implications, that is often misinterpreted from imaging reports. A full explanation is available at what Modic changes on MRI actually mean for your back pain.
From the Clinic: Dr. Arora’s Expert Insight
What consistently trips up powerlifters — more than the injury itself — is the fundamental conflict between how they have trained their entire career and what disc recovery actually demands.
Powerlifters operate under a framework of accumulating load. If it does not hurt badly, do more of it. If it does hurt, reduce volume carefully, manage it, and come back. That logic works reasonably well for tendon adaptations, muscle soreness, and even minor joint irritation. It is the wrong framework for an irritated nerve root, and applying it predictably extends the recovery timeline.
A pattern that comes up repeatedly in this population: a lifter arrives eight or ten weeks post-injury having already tried to push through at reduced intensity — kept squatting, kept doing accessory work, added some stretching from a training forum. Leg symptoms have worsened distally. Pain that was once in the buttock now runs into the calf. The recovery arc is now longer than it needed to be, because the nerve root that required a reduction in mechanical provocation did not receive one.
What generic advice almost always misses is the distinction between reduced load and no load. These are not the same thing, and conflating them causes management to fail in both directions. Complete bed rest is not the protocol. But neither is pushing compound barbell work through active radicular symptoms. The real skill is sequencing the right loads in the right order at the right tissue tolerance — not simply doing less of everything.
The second gap in generic management is treating posterior chain rehabilitation as a pure strengthening problem. It is a sequencing problem. Restoring hip-dominant loading before returning to the barbell is what protects the healing disc. Lifters who return to the platform before that sequencing is established tend to reload the segment before it can tolerate it, and the cycle repeats.
What Should You Do in the First 72 Hours?
In the first 72 hours, the priority is reducing mechanical provocation to the nerve root without entering complete rest. Movement matters — just not loaded spinal movement.
What to Do Today: First 72 Hours
- Reduce load, not all movement. Stop all barbell training immediately. Short walks — 10 to 15 minutes, two to three times per day — maintain circulation and counteract the disc-stiffening effects of sustained inactivity.
- Find your position of relief. Many L5-S1 herniations are more comfortable in mild extension — prone lying, gentle press-ups if tolerated. Others prefer a neutral or slightly flexed position. Use whichever position consistently reduces leg symptoms, not just back pain.
- Avoid sustained loaded flexion. Picking objects off the floor, prolonged sitting, and any forward bending under load are high-irritation postures in the acute phase.
- Manage pain sensibly. Short-term NSAIDs may help reduce nerve root inflammation. Discuss with a prescribing clinician before starting any medication.
- Act immediately if: urinary or bowel changes, saddle numbness, or rapidly progressive bilateral leg weakness develops at any point.
The Powerlifter’s Recovery Protocol: Phase by Phase
L5-S1 herniation recovery for powerlifters is driven by functional milestones, not by elapsed weeks. Progress means the nerve is recovering, the disc is tolerating load incrementally, and the movement patterns underlying the competition lifts have been identified and corrected. Phases overlap in practice — the criteria below are what determine progression, not the calendar.
| Phase | Timeline | Goals | Key Exercises | Progression Criteria |
|---|---|---|---|---|
| 1 — Acute | Weeks 1–4 | Reduce nerve irritation; restore pain-safe movement | Prone press-ups, supine knee-to-chest, gentle walking, diaphragmatic breathing and brace retraining | Leg symptoms begin centralizing — moving toward the back and away from the foot; lying prone is comfortable |
| 2 — Subacute | Weeks 4–10 | Restore hip-dominant movement; begin posterior chain reloading | Glute bridges, clamshells, banded hip abduction, wall-supported hip hinge, bird-dogs, swimming | Hip hinge fully pain-free through range; no increase in leg symptoms during or 24 hours after sessions |
| 3 — Strength Rebuild | Weeks 10–20 | Reload the posterior chain; restore barbell movement competence | Romanian deadlift (light to moderate), goblet squat, trap bar deadlift, cable pull-throughs, landmine press, tempo back squats | Conventional deadlift and squat achievable at 60–70% of pre-injury 1RM without neurological symptom provocation |
| 4 — Return to Competition | Months 5–8+ | Restore competition load; rebuild peaking tolerance | Graduated 1RM testing, competition-specific volume blocks, belt reintegration, full meet-prep cycle | All three competition lifts at pre-injury intensity without symptom recurrence; treating clinician clearance obtained |
On the specific competition lifts:
Trap bar deadlifts and box squats are typically the earliest barbell variants to reintroduce because they allow a more upright trunk position, which reduces the posterior shear moment at L5-S1 compared to conventional pulls and low-bar squats. The conventional deadlift — and the specific technical errors that concentrate load on the lumbosacral segment at the base of the pull — is a late-phase return. A detailed breakdown of the mechanical factors that drive L5-S1 stress during deadlifts is covered in this guide to diagnosing and correcting deadlift-related lower back pain.
The bench press is often assumed to be a safe training outlet during recovery — and frequently it is — but excessive lumbar arch combined with inadequate foot drive can indirectly load the lumbosacral junction. The mechanics relevant to powerlifters are addressed in this guide to bench press and lower back pain.
Restoring gluteal function is a prerequisite for barbell return, not an optional add-on. The glutes are the primary hip extensors in a deadlift and squat, and their inhibition during recovery shifts load back onto the lumbar extensors at precisely the segment that needs protection. The relationship between glute function and lumbar loading during compound lifts is covered in depth at tight glutes and lower back pain.
Do: Keep moving at load levels appropriate to your phase. Use a belt when first returning to barbell work — not as a substitute for bracing, but as a proprioceptive tool during early reload. Prioritize sleep; disc hydration and tissue repair are rest-dependent processes.
Don’t: Load through active leg symptoms, regardless of how manageable the pain feels in the moment. Rush through phases because pain has reduced — the disc is still healing when symptoms improve, and mechanical tolerance has not yet caught up with symptomatic improvement. Use passive therapies (massage, manipulation, heat) as the primary driver of recovery rather than as adjuncts to active rehabilitation.
When Conservative Care Is Not Enough
The majority of lumbar disc herniations — including large ones — improve substantially with structured conservative care over 6–12 weeks. The herniated fragment does not need to return to its original position for recovery to occur. In many cases, the immune system progressively resorbs the displaced nucleus pulposus over months, a natural process that reduces both herniation volume and nerve root irritation without surgical intervention.
Conservative care has reached its clinical limit — and surgical consultation is warranted — when:
- Significant neurological deficit (muscle weakness, reflex loss) is not improving after 6–8 weeks of structured physical therapy
- Pain and functional limitation remain severe after 12 weeks of committed conservative management
- A very large central herniation poses ongoing cauda equina risk regardless of symptom presentation
Microdiscectomy — removal of the herniated disc fragment while leaving the disc body intact — is the most common surgical option for L5-S1 herniation that has not responded to conservative care. A 2021 systematic review and meta-analysis published in Sports Health found that return-to-sport rates were statistically comparable between conservative and surgical management in elite athletes: approximately 81.5% for conservative care versus 83% for surgical intervention, with conservative management achieving this faster on average (Sedrak et al., 2021). Surgery is not inferior when the indication is correct — the outcomes are good. The data simply do not support operating before conservative care has been genuinely trialed.
Post-surgical return to powerlifting is achievable. The rehabilitation phases are structurally the same; the timeline adds approximately 4–6 weeks to the initial recovery phase, and barbell loading is reintroduced more conservatively. Many lifters have competed at a high level after microdiscectomy.
What Can Powerlifters Actually Expect from L5-S1 Herniation Recovery?
The prognosis is better than the acute phase makes it feel. The injury arrives catastrophically — severe leg pain, altered sensation, inability to train — but the natural trajectory of lumbar disc herniation is predominantly one of improvement, particularly in physically robust individuals with high baseline conditioning.
Most powerlifters who manage the recovery correctly will return to structured training within 3–5 months and to competition-level loading within 6–8 months. Those who mismanage the acute phase — typically by continuing to load through active radicular symptoms — extend this timeline significantly. Significant neurological involvement, prior spinal surgeries, and disc degeneration at multiple levels are factors that may lengthen recovery or reduce the likelihood of full return to pre-injury performance.
Realistic phase expectations:
- Weeks 1–4: Pain management, not training. Leg symptoms may fluctuate and temporarily worsen before the improvement trend establishes.
- Months 2–3: Posterior chain activation, hip mechanics, and cardiovascular conditioning. No barbell compounds.
- Months 3–5: Progressive reintroduction of barbell variants under controlled conditions, driven by symptom response rather than fixed timelines.
- Months 5–8: Return to competition-specific loading. Most lifters recover 70–90% of pre-injury strength within this window.
Recurrence is a real risk, particularly at the same disc level, and particularly for lifters who return to the platform without correcting the movement errors and load management practices that contributed to the original injury. Returning to the platform is the milestone; returning without technical correction is the setup for the next one.
Conclusion
An L5-S1 disc herniation is a serious injury. For most powerlifters, it is also a recoverable one. The path back to training — and for many, to competition — is built on accurate understanding of the anatomy, an honest assessment of where symptoms sit on the recovery arc, and a structured protocol that does not confuse symptom reduction with tissue readiness to load. L5-S1 herniation recovery for powerlifters succeeds when the protocol is specific: to the sport’s mechanical demands, to the stage of healing, and to the real functional milestones that determine when the disc can tolerate progressive load again. The lifters who return strongest are almost always those who resisted the urgency to rush, rebuilt the posterior chain properly, and corrected the technical habits that set the stage for the injury in the first place.
Frequently Asked Questions
1. Can I deadlift with an L5-S1 disc herniation?
Not in the acute phase, and not while leg symptoms are active or worsening. The deadlift places the highest compressive and shear load of any common exercise directly on the L5-S1 segment, and loading through an irritated nerve root tends to worsen and prolong symptoms. As nerve function stabilizes and posterior chain mechanics are restored — typically from weeks 10 onwards in a structured protocol — trap bar and Romanian deadlift variants can be reintroduced progressively, with conventional pulls remaining a late-phase return.
2. How long does L5-S1 herniation recovery take for powerlifters?
With a structured conservative protocol, most powerlifters return to training within 3–5 months and to competition-level loading within 6–8 months. The timeline extends when the acute phase is mismanaged — typically by continuing to load through radicular symptoms — or when significant neurological involvement requires a longer nerve recovery arc. Post-surgical cases add approximately 4–6 weeks to each phase of the protocol.
3. Is squatting worse than deadlifting for L5-S1 herniation recovery?
Neither lift is universally worse — the specific mechanics within each movement matter more than the exercise category. Deep squats place L5-S1 in sustained flexion under compression; conventional deadlifts generate high compressive and shear loads at the base of the pull. Both are deferred in the acute and subacute phases. When reintroducing barbell work, trap bar deadlifts and box squats are typically the safer starting points because they permit a more upright torso, which reduces the posterior shear moment at the lumbosacral junction.
4. Will I need surgery for my L5-S1 herniation?
Most people with L5-S1 disc herniations — including those with significant leg symptoms — do not require surgery. Conservative management resolves the majority of presentations when properly structured and sustained. Surgical consultation becomes appropriate when neurological deficits are worsening despite adequate conservative care over 6–8 weeks, or when functional limitation remains severe after 12 weeks of committed rehabilitative effort. Cauda equina symptoms — urinary or bowel changes, saddle numbness — require emergency surgical consultation regardless of how long symptoms have been present.
5. My MRI shows a large herniation. Does that mean a worse recovery?
No. Herniation size on MRI is a consistently poor predictor of both symptom severity and recovery time. Population-based imaging studies have found herniations, bulges, and disc changes in people with no back pain whatsoever. The clinical picture — symptom behaviour, neurological function, centralization pattern, response to position changes — predicts recovery trajectory more accurately than the radiological report. A large-appearing herniation on imaging is not a large-pain prognosis.
6. Can I compete in powerlifting again after an L5-S1 herniation?
Yes, for most athletes. A 2021 systematic review and meta-analysis of elite athletes with lumbar disc herniation found return-to-sport rates of approximately 81.5% with conservative management, with the majority achieving this within 4 months. Powerlifters have a realistic return-to-competition pathway provided the recovery protocol is followed correctly and the movement errors that contributed to the injury are identified and corrected before full competition loading resumes.
7. What movements should I avoid during recovery?
Loaded spinal flexion — conventional deadlifts with significant lumbar rounding, barbell good mornings, heavy rowing in a flexed lumbar position — should be deferred until symptoms have substantially resolved. Sustained forward bending under any load and high-impact activities that generate spinal percussion (running on hard surfaces, jumping) are also deferred in the early and middle phases. As a clinical rule of thumb: any movement that consistently reproduces leg symptoms or pushes them further down the limb should be removed from training until the nerve root has recovered sufficient mechanical tolerance.
Medical Disclaimer
This article is written for general educational purposes and does not constitute medical advice or replace assessment by a qualified healthcare provider. Disc herniation presentations vary significantly between individuals, and recovery timelines depend on factors that require individual clinical evaluation. If you are experiencing progressive neurological symptoms, loss of bladder or bowel control, or bilateral leg weakness, seek emergency medical attention immediately. All rehabilitation protocols described in this article should be adapted under the direct guidance of a physiotherapist or physician who has assessed your specific presentation and imaging findings.
References
- Sedrak P, Shahbaz M, Gohal C, Madden K, Aleem I, Khan M. Return to Play After Symptomatic Lumbar Disc Herniation in Elite Athletes: A Systematic Review and Meta-analysis of Operative Versus Nonoperative Treatment. Sports Health. 2021 Sep-Oct;13(5):446–453. doi: 10.1177/1941738121991782. PMID: 33563131.