Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.
The toddler is almost two. The newborn-fog haze has lifted. You’ve stopped breastfeeding (or you haven’t), you’ve gone back to work (or you haven’t), and life has more or less reorganized itself around a small human who now runs. But one thing has not resolved: your lower back. It nags when you stand at the sink, catches when you bend to scoop up your child, dulls every long drive, and flares whenever you sit too long. Somewhere along the way someone — your mother-in-law, a coworker, a forum thread at 2 a.m. — said the words: it must be the epidural.
That theory is everywhere. And once it lodges, it’s hard to dislodge.
Here is the uncomfortable truth: lower back pain 2 years after epidural is real, common, and worth taking seriously — but the epidural itself is almost never the cause. Decades of randomized trial data show no causal link between epidural analgesia during childbirth and long-term backache. What is actually causing the pain is usually something else entirely, and it is something physical therapy (physiotherapy) can address. This article walks through what the evidence actually shows, what is far more likely driving your symptoms, and what to do about it starting this week.
Key Takeaways
- Large randomized trials and a major Cochrane systematic review have found no causal link between epidural analgesia during labor and long-term lower back pain.
- The two-year mark is when many women first realize their pain isn’t going to “just resolve” on its own — but the driver is usually postpartum biomechanics, not the injection.
- Common real culprits include sacroiliac joint dysfunction, abdominal wall changes (including diastasis recti), deconditioned trunk and hip muscles, asymmetric childcare loading, and pre-existing issues that pregnancy revealed.
- Most cases respond well to targeted physical therapy. Imaging is rarely needed in the first 4–6 weeks of structured rehab.
- Red flags — leg weakness, saddle numbness, bladder or bowel changes, unexplained weight loss, night pain that wakes you — warrant urgent medical assessment, regardless of when they appear.

What does “lower back pain 2 years after epidural” usually turn out to be?
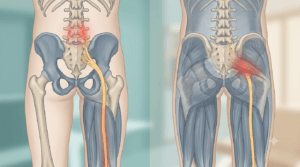
In the clinic, this presentation has a recognizable shape. The pain typically sits low and central, sometimes drifting toward one side or into the buttock. It is worse with prolonged sitting, prolonged standing, and the specific moments of postpartum life — lifting a car seat from the back of a vehicle, leaning over a bath, carrying a child on one hip while cooking, or hunching to feed in a low chair. It rarely behaves like nerve pain shooting down the leg. It almost never behaves like the sharp, localized tenderness of an actual epidural injection site, which would have resolved within days to weeks.
The reason women blame the injection is intuitive: that needle went into the spine, the pain is in the spine, the timeline started after that day. Correlation feels like causation. But two years is a long time. In two years, the body has carried, birthed, fed, lifted, twisted, sat on the floor, gotten back into shape (or hasn’t), returned to work, returned to exercise (or hasn’t), and built thousands of new movement habits — many of them asymmetrical, many of them imposed by the practical realities of motherhood. The driver of the pain almost certainly lives in those habits, not in a needle from 2023 or 2024.
Lower Back Pain 2 Years After Epidural: What the Evidence Actually Says
The strongest evidence on this question comes from prospective randomized trials and a major systematic review — and the finding is unusually consistent.
A landmark BMJ study randomized women to either epidural or non-epidural analgesia during labor and assessed them at three months, twelve months, and two years after delivery. The researchers concluded that there was no evidence of a causal link between epidural analgesia during labour and low back pain (Howell et al., 2002). The two-year follow-up timing matters here: it is exactly the window in which thousands of women a year arrive at clinics blaming an injection.
The most authoritative pooled evidence is a Cochrane systematic review of forty trials involving over eleven thousand women, comparing epidural with non-epidural pain relief during labor. The review reported little or no difference in the number of women with long-term backache between the two groups (Anim-Somuah et al., 2018). In plain language: women who have epidurals and women who don’t develop long-term back pain at essentially the same rate.
That doesn’t mean nothing can go wrong with an epidural. Localized tenderness at the injection site for a few days is normal. True complications — persistent nerve injury, infection, hematoma — are rare and almost always declare themselves within days or weeks of the procedure, not years later. A pain that appeared during pregnancy, persisted through the postpartum year, and is still bothering you now is, statistically, a postpartum musculoskeletal problem that has been misattributed.
This is good news. A condition without a clear cause is hard to treat. A condition that has been mis-blamed on something untreatable becomes treatable the moment you correctly identify the actual driver.
What’s actually causing the pain? Anatomy and biomechanics two years on
Pregnancy and childbirth do not just leave a baby behind. They leave a transformed musculoskeletal system, and the changes do not fully reverse on their own.
During pregnancy, the hormone relaxin softens the ligaments of the pelvis to allow the baby to pass through. The lumbar spine adopts a more extended posture to accommodate the growing belly. The abdominal wall stretches — sometimes to the point of midline separation (diastasis recti). The pelvic floor is loaded for nine months and then, in vaginal delivery, stretched dramatically. The deep stabilizing muscles of the trunk — transverse abdominis, multifidus, pelvic floor, diaphragm — frequently switch off or coordinate poorly in the months that follow.
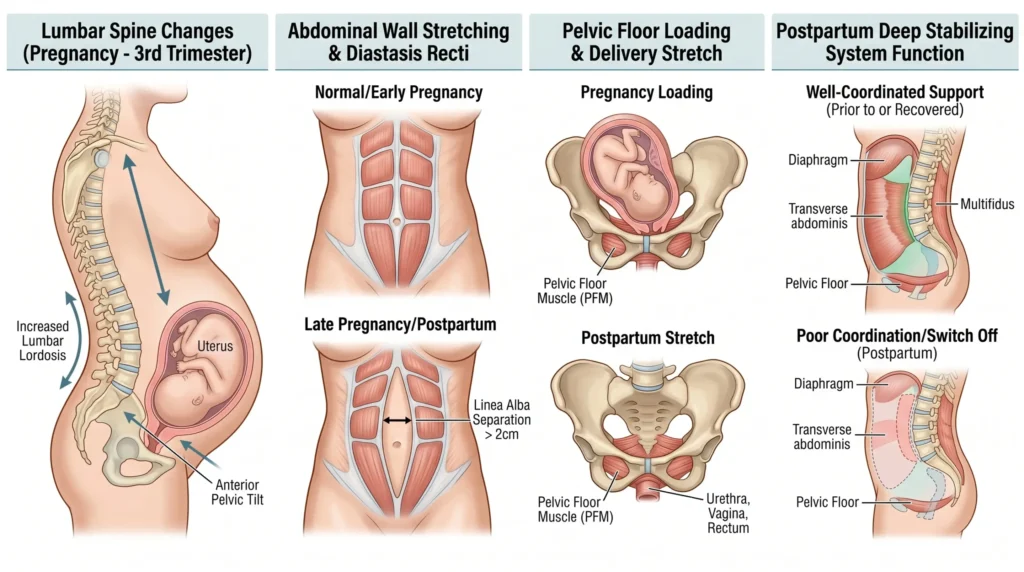
This image is for representational and educational purposes only. It is not intended to serve as or replace professional medical advice, diagnosis, or treatment.
After birth, the demands change again. You carry a baby on one side, then the other, then back to the dominant side. You lift a car seat from awkward angles. You sit hunched while feeding for hours every day. You sleep in odd positions to soothe a crying infant. You stop the gym you used to do and may or may not return to it. By the time your child is two, the nervous system has thoroughly learned a new pattern of moving — and that pattern is rarely a friendly one for the lower back.
This is the same story for women who never had an epidural, women who had a cesarean, and women who labored without anesthesia. The driver isn’t a needle. The driver is the cumulative effect of pregnancy, birth, and the daily mechanics of parenting on a back that didn’t get a structured rehab program. For a closer look at how this plays out after a different delivery route, this companion article on persistent back pain a year after a C-section covers the parallel mechanism.
What else commonly drives this pattern? (Differential thinking)
When a woman walks in describing lower back pain two years after epidural, the working differential is rarely “epidural-induced spinal pathology.” It is usually one of a handful of treatable patterns. The table below maps the patterns most often missed in routine assessment.
| What it feels like | What it might be | Why two years later |
|---|---|---|
| Deep ache low and central, worse with prolonged sitting and standing, better with walking | Lumbar deconditioning + altered movement patterns | Trunk and hip stabilizers never got formally retrained postpartum |
| Sharp pinch low on one side, worse with rolling in bed, climbing stairs, getting in/out of a car | Sacroiliac joint dysfunction | Pelvic ligaments softened by relaxin never regained full tension; one side now overworks |
| Doming or coning of the midline of the abdomen when sitting up; back fatigues quickly | Diastasis recti / abdominal wall dysfunction | The deep core has not been reorganized; the back is doing the work the abdominals should |
| Pain that flares when carrying the child, especially on one hip | Asymmetric load tolerance + weak hip abductors | Two years of one-sided carrying has built a deeply learned asymmetry |
| Pain that started in pregnancy and never fully went away | Pre-existing low-grade lumbar issue, exposed by pregnancy load | The pregnancy made a borderline problem symptomatic; postpartum life keeps it that way |
| Heaviness or dragging sensation low in the abdomen along with back pain | Possible pelvic floor or pelvic organ involvement | Pelvic floor strength has not been formally addressed |
The point of this differential is not self-diagnosis. It is to help you stop looking up at your spine — and start looking at how your trunk, pelvis, hips, and pelvic floor are actually working as a system. For a broader picture of why women in particular develop this kind of persistent back pain, this overview of common causes in women is a useful companion read.
When could it actually be related to the epidural? And what should genuinely worry me?
The short answer is: very rarely, and almost never two years later. Localized tenderness at the puncture site can persist for a few days, occasionally a few weeks. Persistent neurological symptoms — leg weakness, numbness in a specific dermatomal pattern, bladder or bowel disturbance, saddle numbness — are uncommon complications and would have surfaced soon after the procedure, not after two years of otherwise normal function.
Far more important than the epidural question are the general red flags that warrant urgent assessment regardless of cause or timing:
⚠️ Seek care urgently if you experience:
- New or worsening weakness in one or both legs
- Numbness in the area that would touch a saddle (inner thighs, buttocks, genitals)
- New loss of bladder control, or new difficulty emptying the bladder
- New loss of bowel control, or unexplained constipation with back pain
- Unexplained weight loss, fever, or night sweats with back pain
- Pain that wakes you from sleep and is unrelieved by changing position
- Back pain following recent significant trauma
These features are not specific to postpartum or post-epidural pain. They are reasons to be seen urgently no matter who you are.
Do I need an MRI?
Almost certainly not — at least not yet. For uncomplicated postpartum lower back pain, imaging in the first month or two of structured rehab rarely changes management. An MRI in a healthy adult will frequently show disc bulges, mild degenerative changes, and minor signal abnormalities that are also present in pain-free people of the same age. Finding something on a scan does not mean that something is the cause of pain. It often makes the situation worse by anchoring fear to an image.
Imaging becomes genuinely useful when:
- Red flags are present
- Symptoms are clearly neurological (significant leg weakness, true radicular pain in a specific nerve distribution)
- A structured 4–6 week rehab program has failed and the clinical picture is atypical
- A specific surgical question is being asked
If the pain is mechanical (changes with position and movement), responds to load and rest in predictable ways, and is not accompanied by red flags, the most accurate “test” is a careful in-person assessment of how the trunk, pelvis, and hips actually move.
From the Clinic: Dr. Arora’s Expert Insight
If there is one conversation that comes up almost weekly in postpartum back pain assessments, it is this one: a woman walks in convinced her pain is from the epidural, and she has been carrying that belief for two years like a verdict. Many have already had imaging that came back essentially normal, which made things worse rather than better — because if nothing structural is wrong but the pain is real, the explanation must be something nobody else has spotted, and the epidural becomes the lingering suspect.
What shows up again and again is the same clinical pattern. The deep abdominal wall is not engaging properly. The pelvic floor has not been formally rehabilitated. The hip abductors on at least one side are weak — usually the side the child is carried on. The thoracic spine has lost rotation, so the lumbar spine compensates with extra movement on every twist and reach. And the entire trunk has learned to brace inefficiently. None of this is visible on an MRI. All of it is treatable.
The failure mode I see most often with generic advice is well-intentioned but unhelpful — “do more core work” usually means crunches and planks, which can actively worsen abdominal wall dysfunction in the postpartum population. What works is the opposite order: restore the deep system first (breathing, transverse abdominis, pelvic floor, diaphragm working together), then layer hip and glute work, then progress to loaded patterns, and only then progress to higher-impact return to activity. A reader who has been told her back is “just weak” and given a generic strengthening sheet has almost always been given the wrong starting point.
When I sit with someone two years postpartum and we trace the actual mechanics — what muscles fire when, what compensations have set in, what daily habits keep reinforcing the asymmetry — the picture is almost never one of epidural injury. It is the picture of a body that did extraordinary work, never got a proper handover back into normal function, and has been quietly compensating ever since. That is a very different problem, and it has a very different solution.
What should I actually do today?
✅ What to do this week
- Stop catastrophizing the spine. The pain is real, but the structure is almost certainly fine.
- Walk daily. Start with 15–20 minutes (about 1.5 km / 1 mile) at an easy pace and build from there. Movement is the most consistently effective early intervention.
- Audit carrying habits. For one day, notice which hip you put the child on, which arm carries the car seat, and which side you sleep on. Begin alternating consciously.
- Address sitting. If you feed, work, or scroll for long stretches, change position every 25–30 minutes, even briefly.
- Try a gentle hip-hinge pattern. Stand with feet hip-width apart, push the hips back as if closing a drawer with your behind, keep the spine long, and return. Five sets of eight, twice a day, is enough to begin.
- Book a postpartum-trained physiotherapist assessment if pain has been ongoing for more than a month or is limiting daily activity.
For the first 48–72 hours of a flare-up, gentle heat is usually more useful than ice in this presentation because the dominant problem is muscular guarding and stiffness, not acute inflammation — though the choice between ice and heat depends on the specific scenario.
Phase-by-phase rehab: how the rebuild actually works
Recovery is not a single exercise. It is a sequence. Trying to skip the early phases — which is exactly what generic programs do — is why so many women feel like nothing works.
| Phase | Time frame | Goal | What it looks like | When to advance |
|---|---|---|---|---|
| 1. Reset the deep system | Weeks 1–2 | Restore coordination of diaphragm, transverse abdominis, and pelvic floor | 360° breathing; gentle pelvic floor + transverse abdominis activation; supine pelvic tilts; cat–camel | Can engage the deep core without holding the breath or doming the abdomen |
| 2. Hip and glute foundation | Weeks 2–4 | Wake up the hip stabilizers that asymmetric loading has weakened | Side-lying hip abduction; glute bridges; clamshells; single-leg balance | Can stand on one leg for 30 seconds without trunk shift; pain reducing |
| 3. Hinge and load | Weeks 3–6 | Train the back and hips to handle real-life lifting | Hip-hinge progressions; supported deadlift patterns with light load (5–10 kg / 10–20 lb); kettlebell work | Can lift a 10 kg / 20 lb load from floor to hip without pain or compensation |
| 4. Functional reload | Weeks 6–10 | Translate gym work into life mechanics | Carrying the child with intent; loaded carries; squat-to-stand from the floor; return to running, cycling, or gym | Can carry the child or a 15 kg / 30 lb load for 5 minutes without back fatigue |
| 5. Long-term resilience | Ongoing | Build a baseline of strength that absorbs the chaos of parenting | Twice-weekly strength work targeting hinge, squat, push, pull, carry | This phase doesn’t end — it becomes maintenance |
Most women see meaningful improvement by week 4–6 if they actually do the work in order. A step-by-step home program built around this kind of sequencing is a useful starting point for readers who want a structured plan to follow.
What makes it worse and what to avoid
Some of the most well-intentioned advice quietly makes postpartum back pain worse.

Avoid in the early phase:
- Crunches, sit-ups, and traditional planks before the abdominal wall is reorganized
- Generic “core” classes that load the spine into flexion or rotation without screening
- Prolonged sitting in deep slouched postures while feeding or scrolling
- Always carrying the child on the same side
- “Pushing through” exercise that consistently flares the back for hours afterwards
Do more of:
- Walk daily, every day, even if briefly
- Breath-led core engagement before any abdominal work
- Hip and glute strengthening, both sides equally
- Hip-hinge mechanics for every lift, every time
- Strength work twice a week — the postpartum body responds to loading, not just stretching
Breastfeeding posture and the load of carrying influence the spine in ways that are easy to overlook. Women with larger breasts often carry an additional load pattern that interacts with postpartum back changes; this article on lower back pain and breast load explores that overlap in more detail.
When does conservative care fail, and what comes next?
Conservative care for postpartum lower back pain is highly effective, but not universally and not always quickly. A reasonable benchmark is meaningful improvement within 6–8 weeks of consistent, well-targeted rehab. “Meaningful” does not mean “completely pain-free” — it means the pain is less frequent, less intense, less limiting, and function is measurably better.
If, after a genuine 6–8 week effort with a skilled clinician, the picture is unchanged, the next steps are:
- Detailed re-assessment. Often the original working diagnosis was incomplete. Pelvic floor involvement, hip joint pathology, or sacroiliac joint dysfunction may have been under-treated.
- Targeted imaging. At this point an MRI may genuinely add information, especially if the clinical picture is atypical or features have changed.
- Specialist referral. A spine physician, women’s health physician, or pelvic medicine specialist may be appropriate depending on what the reassessment reveals.
Surgery has essentially no role in uncomplicated postpartum mechanical back pain. It is reserved for specific surgical pathology — significant nerve compression with neurological deficit, or structural instability — and that is rarely what this presentation is.
Realistic outlook
Lower back pain 2 years after epidural is, in the vast majority of cases, postpartum mechanical pain that was never given a proper rehab program. The outlook with structured care is genuinely good. Most women regain full function. Many end up stronger than they were before pregnancy, because the rehab process forces them to address weaknesses that were always there but never demanded attention. The two-year mark is not a deadline. It is simply the moment when many women decide they are done waiting for the pain to fix itself.
The epidural is not the enemy. The lack of a real recovery plan is.
Frequently Asked Questions
1. Can an epidural cause back pain years later?
No reliable evidence supports this. The most authoritative randomized trials and a Cochrane systematic review of over eleven thousand women have not found a causal link between epidural analgesia during labor and long-term backache. Localized tenderness at the injection site, when it happens, resolves within days to a few weeks.
2. Why does my back hurt only on one side two years after an epidural?
One-sided lower back pain after childbirth is almost always asymmetric loading: carrying the child on one hip, sleeping on one side to soothe an infant, or weakness in one hip stabilizer driving compensation through the back. Sacroiliac joint dysfunction is a common contributor to this pattern.
3. Is it normal to still have postpartum back pain after two years?
Common is not the same as normal. Persistent pain at two years is a signal that the postpartum musculoskeletal system has not been formally rehabilitated. It usually responds well to targeted physical therapy. It should not be accepted as the new baseline.
4. Could I have permanent nerve damage from my epidural?
Permanent nerve injury from epidural anesthesia is rare, and it almost always presents within days or weeks of the procedure as clear neurological symptoms — significant leg weakness, sensory loss in a defined area, or bladder or bowel problems. A back ache that has waxed and waned over two years without any of those features is not a nerve injury from the epidural.
5. Will an MRI tell me what’s wrong?
Often, it tells you less than you’d expect. MRIs in healthy adults frequently show disc bulges and minor degenerative findings that are also present in people with no pain. A skilled in-person assessment of how the trunk, pelvis, and hips move is usually more informative for this presentation than an early scan.
6. Can I get back into the gym or running with this kind of pain?
Yes — in the right sequence. Most women can safely return to running, lifting, and high-impact training, but skipping straight back to it without restoring the deep core, hip strength, and hinge mechanics is exactly what keeps the pain going. The four-phase rehab structure above is the route.
7. How long will it take to fix this?
A realistic expectation is meaningful improvement in 4–6 weeks of consistent, well-targeted work, with substantial recovery typically within 8–12 weeks. The pain may not be completely gone in that window, but its frequency, intensity, and limiting effect should be visibly reducing.
8. Should I be worried that no one has been able to fix it so far?
Not necessarily. Postpartum back pain is often under-treated because the assessment skips the deep core, pelvic floor, and asymmetric loading patterns and goes straight to “strengthen the back.” A clinician who specifically works with the postpartum population usually approaches it very differently.
{ “@context”: “https://schema.org”, “@type”: “FAQPage”, “mainEntity”: [ { “@type”: “Question”, “name”: “Can an epidural cause back pain years later?”, “acceptedAnswer”: { “@type”: “Answer”, “text”: “No reliable evidence supports this. The most authoritative randomized trials and a Cochrane systematic review of over eleven thousand women have not found a causal link between epidural analgesia during labor and long-term backache. Localized tenderness at the injection site, when it happens, resolves within days to a few weeks.” } }, { “@type”: “Question”, “name”: “Why does my back hurt only on one side two years after an epidural?”, “acceptedAnswer”: { “@type”: “Answer”, “text”: “One-sided lower back pain after childbirth is almost always asymmetric loading: carrying the child on one hip, sleeping on one side to soothe an infant, or weakness in one hip stabilizer driving compensation through the back. Sacroiliac joint dysfunction is a common contributor to this pattern.” } }, { “@type”: “Question”, “name”: “Is it normal to still have postpartum back pain after two years?”, “acceptedAnswer”: { “@type”: “Answer”, “text”: “Common is not the same as normal. Persistent pain at two years is a signal that the postpartum musculoskeletal system has not been formally rehabilitated. It usually responds well to targeted physical therapy and should not be accepted as the new baseline.” } }, { “@type”: “Question”, “name”: “Could I have permanent nerve damage from my epidural?”, “acceptedAnswer”: { “@type”: “Answer”, “text”: “Permanent nerve injury from epidural anesthesia is rare, and it almost always presents within days or weeks of the procedure as clear neurological symptoms — significant leg weakness, sensory loss in a defined area, or bladder or bowel problems. A back ache that has waxed and waned over two years without any of those features is not a nerve injury from the epidural.” } }, { “@type”: “Question”, “name”: “Will an MRI tell me what’s wrong?”, “acceptedAnswer”: { “@type”: “Answer”, “text”: “Often, it tells you less than you’d expect. MRIs in healthy adults frequently show disc bulges and minor degenerative findings that are also present in people with no pain. A skilled in-person assessment of how the trunk, pelvis, and hips move is usually more informative for this presentation than an early scan.” } }, { “@type”: “Question”, “name”: “Can I get back into the gym or running with this kind of pain?”, “acceptedAnswer”: { “@type”: “Answer”, “text”: “Yes — in the right sequence. Most women can safely return to running, lifting, and high-impact training, but skipping straight back to it without restoring the deep core, hip strength, and hinge mechanics is exactly what keeps the pain going. A staged four-phase rehab structure is the route.” } }, { “@type”: “Question”, “name”: “How long will it take to fix this?”, “acceptedAnswer”: { “@type”: “Answer”, “text”: “A realistic expectation is meaningful improvement in 4–6 weeks of consistent, well-targeted work, with substantial recovery typically within 8–12 weeks. The pain may not be completely gone in that window, but its frequency, intensity, and limiting effect should be visibly reducing.” } }, { “@type”: “Question”, “name”: “Should I be worried that no one has been able to fix it so far?”, “acceptedAnswer”: { “@type”: “Answer”, “text”: “Not necessarily. Postpartum back pain is often under-treated because the assessment skips the deep core, pelvic floor, and asymmetric loading patterns and goes straight to ‘strengthen the back.’ A clinician who specifically works with the postpartum population usually approaches it very differently.” } } ] }Medical Disclaimer
This article is intended for general educational purposes and does not replace personalized medical assessment. If symptoms are worsening, accompanied by neurological changes, or limiting daily life, please seek in-person evaluation from a qualified clinician. Questions about anesthetic procedures should be discussed directly with an anesthesiologist or the obstetric team that managed the delivery.
References
- Howell CJ, Dean T, Lucking L, Dziedzic K, Jones PW, Johanson RB. Randomised study of long term outcome after epidural versus non-epidural analgesia during labour. BMJ. 2002;325(7360):357. doi:10.1136/bmj.325.7360.357. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC117883/
- Anim-Somuah M, Smyth RMD, Cyna AM, Cuthbert A. Epidural versus non-epidural or no analgesia for pain management in labour. Cochrane Database of Systematic Reviews. 2018;5:CD000331. doi:10.1002/14651858.CD000331.pub4. Available at: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD000331.pub4/full