“Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.”
There is a conversation that happens quietly in a lot of physiotherapy waiting rooms. A woman mentions her back pain to her GP, gets told to work on her posture and strengthen her core, tries both diligently for months, and sees marginal improvement at best. What frequently goes unaddressed is the structural reality that her chest is carrying several additional kilograms in front of her spine — all day, every day — and no amount of core work is going to neutralize that if the management plan doesn’t account for it.
Lower back pain from large breasts is a genuine, well-documented clinical problem. It is more common than the medical community once acknowledged, more mechanically interesting than the oversimplified “your chest is heavy” explanation suggests, and far more manageable through targeted conservative care than most women are told.
This article explains what is actually happening in the spine when breast weight becomes a driver of lower back pain, how to distinguish this from other causes of back pain in women, what physical therapy (physiotherapy) can realistically achieve, and when surgical reduction deserves an honest conversation.
Key Takeaways
- Large breasts shift the body’s center of gravity forward, increasing compressive load on the lumbar spine and fatiguing the muscles that hold you upright.
- The pain is typically dull, bilateral, and worse after prolonged standing or walking — it tends to ease when you lie down.
- A properly fitted supportive bra, posterior chain strengthening, and postural retraining can produce significant relief, but the exercise selection matters.
- Imaging is rarely needed in straightforward cases; it becomes relevant when conservative management fails or neurological symptoms develop.
- Breast reduction surgery (reduction mammoplasty) has meaningful evidence supporting its use when conservative measures have been properly exhausted and breast volume is the dominant mechanical driver.

The Spinal Load Problem: What’s Actually Happening
Your lumbar spine — the lower five vertebrae — is built to handle load that shifts dynamically with movement: sitting, walking, lifting, reaching. What it tolerates less well is a persistent, static, anteriorly-placed mass pulling it out of alignment for hours at a stretch.
Large breasts increase the tissue mass positioned in front of the spine and above the waist. When that anterior load is significant — whether from macromastia (clinically disproportionate breast hypertrophy), weight gain, or hormonal changes that increase glandular volume — the body compensates through a predictable chain of postural adjustments.
The thoracic spine, which sits directly behind the chest, tends toward greater kyphosis (forward rounding) as the weight pulls anteriorly. To keep the head upright and the eyes level, the cervical spine shifts forward — the familiar forward head posture. At the lumbar level, the spine often increases its lordosis (the inward curve of the lower back) to shift the body’s center of gravity back over the pelvis. This compensatory hyperlordosis raises the mechanical demand on the lumbar facet joints and the surrounding musculature.
The paraspinal muscles — particularly the erector spinae, running in columns along either side of the spine — are responsible for maintaining upright posture against this forward pull. In women with significant breast weight, these muscles are effectively doing overtime. Over time, chronic fatigue accumulates at the muscular level, and the facet joints begin absorbing more load than they are designed to sustain. The result is familiar: a persistent, often bilateral ache across the lower back that worsens with standing or walking and eases only with lying down.
The thoracolumbar fascia — a broad sheet of connective tissue that wraps the lower back muscles and transfers force across the spine and pelvis — is also implicated. Chronic overload of this structure contributes to the early-morning stiffness and deep, hard-to-place ache that many women with this pattern describe.
Why Lower Back Pain from Large Breasts Develops
Large breasts shift the body’s center of gravity forward, increasing rotational torque at the lumbar spine and forcing the paraspinal muscles to work continuously against that anterior load. Over time, this produces muscle fatigue, compensatory changes in spinal alignment, and pain that is reliably worse after any prolonged upright activity.
A woman with a D cup or larger may be carrying anywhere from 500 grams to over 2 kilograms (approximately 1 to 4.5 lbs) of additional tissue positioned anteriorly on her thorax. That may sound modest, but because of the lever arm involved — the distance between the breast tissue and the lumbar spine — even moderate breast weight generates a disproportionately large rotational moment at the lower back. The spinal muscles must produce a continuous counterforce to prevent forward spinal collapse.

Bra fit compounds this considerably. An ill-fitting or unsupportive bra concentrates most of the breast load onto the shoulder straps. The trapezius and levator scapulae work to resist that downward strap traction, creating a secondary chain of cervicothoracic tension that can refer pain well below the shoulder girdle and contribute to mid- and lower-back symptoms throughout the day.
Not every woman with large breasts develops significant back pain — and this is clinically important to understand. Core strength, pelvic alignment, occupation, footwear, fitness level, and body composition all influence how well the spine tolerates the anterior load. A woman who is physically active, has good posterior chain strength, and wears a well-fitted supportive bra may experience little more than mild fatigue at day’s end. A woman with the same cup size who sits for eight hours, wears an unsupported bra, and has weak hip extensors may find herself in near-constant pain by mid-afternoon.
How the Pain Typically Presents
Lower back pain associated with significant breast weight has a recognizable clinical pattern. It tends to be bilateral — across both sides of the lower back rather than distinctly one-sided, though one side may be more prominent if postural asymmetry or mild scoliosis is present. It is reliably positional: worse with prolonged standing, walking, or any sustained upright activity, and meaningfully better with lying down. The quality is typically dull and deep — a dragging fatigue-type ache rather than a sharp or stabbing sensation — and it is frequently accompanied by thoracic stiffness, trapezius tightness, or neck aching that develops alongside the lower back symptoms as the day progresses.
Pain that radiates down one or both legs, causes numbness or tingling below the knee, does not change at all with position, or is associated with any bladder or bowel changes does not fit this mechanical pattern and warrants proper assessment before being attributed to breast size.
When It’s Not Just Breast Weight: Thinking Through the Differentials
Lower back pain in women has a broader differential than is often appreciated, and breast size — even when genuinely contributing — rarely operates in complete isolation.
Sacroiliac joint dysfunction is commonly overlooked in this population. The SI joint connects the sacrum to the pelvis and is frequently irritated by altered gait mechanics and asymmetric postural loading — both of which are more common in women with macromastia. SI joint pain typically presents as a deep ache in the lower back or buttock on one side, provoked by rolling over in bed, stair-climbing, or prolonged single-leg standing.
Lumbar disc involvement can develop alongside macromastia-related loading rather than independently of it. Compensatory lumbar hyperlordosis increases posterior disc and facet loading, which over time may contribute to disc degeneration or, less commonly, disc herniation. If leg pain, calf weakness, or foot tingling accompanies the back symptoms, a nerve root component needs to be assessed and should not be assumed to be breast-related.
Myofascial pain syndrome — chronic trigger points within the thoracic erectors, rhomboids, or quadratus lumborum — is extremely common in this group. These trigger points develop as a direct response to sustained postural overload and can generate both local and referred lower-back pain that is easily misattributed to spinal pathology.
Non-musculoskeletal causes deserve consideration in any woman with lower back pain. Endometriosis, uterine fibroids, ovarian pathology, and pelvic inflammatory disease can all produce low back pain that is easy to attribute to posture. If the pain has no clear postural or movement relationship, occurs cyclically, or is associated with pelvic or gynaecological symptoms, investigation beyond the musculoskeletal system is appropriate — regardless of breast size.
Red Flags: When to Seek Prompt Medical Attention
For most women, lower back pain related to breast weight is a mechanical problem and not medically urgent. However, specific symptoms require prompt evaluation and should not be attributed to posture without proper assessment:
- Saddle anesthesia — numbness or tingling in the inner thighs, groin, or perineal area alongside back pain — is a neurological emergency. This combination suggests cauda equina syndrome and requires same-day hospital assessment.
- Progressive leg weakness that is measurably deteriorating over days or weeks, rather than fluctuating with activity levels, warrants urgent imaging to assess nerve root compression.
- Back pain alongside unexplained weight loss, drenching night sweats, persistent fever, or a personal or family history of cancer requires investigation to exclude a systemic or oncological cause. This type of pain typically does not vary with posture.
- Constant, unrelenting pain that does not ease in any position, including lying flat, is not consistent with mechanical back pain and needs assessment.
Imaging: When It Actually Changes the Picture
In straightforward cases of lower back pain from large breasts, imaging rarely contributes useful information to the initial management plan. An X-ray will likely demonstrate increased lumbar lordosis — which a clinical posture assessment can identify without radiation. An MRI may reveal disc changes that are present in a large proportion of women in the same age range regardless of breast size, and finding those changes does not automatically explain the pain or direct a different course of treatment.
The right question before ordering any imaging is: will the result change what happens next? If the management plan stays the same regardless of the scan, the scan is not yet indicated.
Imaging becomes genuinely useful when neurological symptoms suggest nerve root compression that needs to be located and graded; when red flag symptoms require exclusion of serious pathology; when conservative management has been properly delivered for three or more months without meaningful improvement and a surgical or injection-based option is under consideration; or when breast reduction surgery is being planned and the surgeon requires spinal baseline data as part of their pre-operative assessment.
Common Misconceptions Worth Addressing
“Losing weight will fix it.” Weight management is relevant and can reduce breast volume in some women, but for many — particularly those with predominantly glandular rather than fatty breast hypertrophy — breast size is not primarily driven by body weight. Exercise-based weight loss may not meaningfully reduce breast mass. Some women who lose significant body weight find their breast-to-frame ratio actually increases as general fat reduces but glandular tissue remains.

“A sports bra is the best support option.” Not necessarily. A compression sports bra reduces movement during activity but can create significant anterior thoracic pressure and worsen postural load when worn throughout the day. An encapsulating bra with wide, padded shoulder straps, a stable underwire that follows the chest wall contour, and a firm band provides meaningfully better everyday load distribution.
“Strengthening the core will sort it out.” Targeted core work is genuinely useful, but prescribing generic abdominal exercises without addressing the posterior chain — the glutes, thoracic extensors, and deep spinal stabilizers — consistently underdelivers. The problem is not simply a weak front; it is an imbalance between an anteriorly overloaded thorax and an undertrained posterior system that lacks the capacity to counterbalance it.
“This is just what it’s like having a large chest.” It is not. Chronic lower back pain is not an inevitable consequence of large breast size. It is a mechanical problem with identifiable, addressable contributors. Many women achieve lasting relief without surgery — but that outcome requires targeted management, not resignation.
From the Clinic: Dr. Arora’s Expert Insight
Patient comes and tells me that I am having low back pain, i went to ortho and GP they said I have weak core, needs straightening — and then the patient sits down and you I immediately that posture is downstream of something nobody has actually assessed yet.
What I encounter consistently in clinic is that these women have been offered a narrow set of options: generic core exercises, a mention that weight loss might help, and occasionally a suggestion to get a bra fitting. None of these are wrong, but they are incomplete in a way that costs months of progress. The generic core exercises almost always emphasize the anterior chain — crunches, planks, dead lifts in a flexed spine — and do nothing to rebuild the thoracic extensors, lower trapezius, and posterior shoulder girdle that are being continuously eclipsed by the forward load from the front. It is the equivalent of trying to stabilize a heavy door that pulls open by only strengthening the door frame on the inside.
What actually shifts outcomes, conservatively, is loading the posterior chain specifically. The goal is not to cancel out the anterior load — you cannot — but to build enough posterior capacity that the spine stops being progressively fatigued by it. That shift takes time: typically eight to twelve weeks of consistent, well-chosen exercise. The improvement, when the programme is right, can be substantial.
The other thing I want to be direct about: breast reduction surgery, when conservative care has genuinely failed, is not a cosmetic decision in these cases. It is a structural intervention for a load-driven mechanical problem, and the evidence supports it. Women who have carried this pain for years sometimes tell me they wished the surgical option had been framed that way from the beginning — not as a last resort after repeated rounds of under-targeted physiotherapy, but as a legitimate clinical pathway alongside it.
Managing the Pain: A Practical Approach
The First 48–72 Hours of a Flare
If the lower back is acutely flared — stiff, achy, resistant to movement — the first priority is offloading rather than active treatment. Short rest periods of 30 to 60 minutes in a supported supine position with knees bent help reduce paraspinal muscle guarding without promoting prolonged inactivity. Heat applied to the lower back for 15 to 20 minutes tends to relieve muscle-driven pain more effectively than ice in these cases. Short-term use of an anti-inflammatory medication can be appropriate if there are no contraindications, but should not become the default ongoing management strategy.
This is also the time to honestly review bra support. A flare that coincides with a change in bra, an unsupported long day, or a high-impact activity in inadequate support is a useful clinical clue about what is driving the pain.
Phase-Based Rehabilitation
Phase 1 — Reducing load and restoring movement (Weeks 1–2)
The first priority is reducing compressive and postural demand on the lower back without simply stopping all activity. Walking with good hip extension, supported sitting with a small lumbar roll placed at the hollow of the back, and basic diaphragmatic breathing that gently engages the deep stabilizing muscles without loading the lumbar spine are appropriate starting points. This phase is also the right time to address bra support properly — a professional fitting, not a rushed approximation.
Gentle thoracic mobility work begins here as well: seated thoracic rotations with the arms crossed, prone thoracic extensions over a rolled towel, or a supported thoracic extension over a foam roller. These counteract the kyphotic rounding that forward breast load drives, without demanding strength from muscles that are not yet ready to be loaded.
Phase 2 — Building posterior chain capacity (Weeks 3–8)
This is the clinical core of conservative management. The exercises most likely to produce lasting benefit are those that load the posterior chain in a way that directly offsets the anterior thoracic pull:
- Prone Y, T, and W drills — These recruit the lower trapezius and mid-thoracic extensors with low spinal load. They are easily underestimated and produce disproportionate benefit in this clinical pattern.
- Glute bridges and hip thrusts — Building gluteal capacity restores lumbopelvic mechanics and reduces the lumbar facet loading that contributes to the daily aching pattern.
- Banded or cable rows — Mid-row variations that train scapular retraction and thoracic extension simultaneously address the rounded shoulder pattern that anterior breast load progressively drives.
- Dead bugs — A supine exercise that builds deep lumbar stabilizer capacity (multifidus, transverse abdominis) without placing the spine in a loaded flexed position.
- Hip hinge training — Teaching the hip hinge movement — bending forward by folding at the hips rather than flexing the lumbar spine — is critical for daily tasks like picking things up, loading the dishwasher, or leaning over a child.
Progression within this phase should be guided by symptom response: exercises that produce mild muscular fatigue but no increase in back pain during or in the 24 hours following are appropriate. For a structured home exercise framework that complements this phase, the Low Back Pain Exercises Physical Therapy step-by-step program provides a well-sequenced starting point. The 7 Low Back Pain Exercises Physical Therapists Swear By offers additional options that integrate well alongside posterior chain loading.
Phase 3 — Load tolerance and return to full activity (Weeks 8–16)
As pain reduces and posterior capacity improves, the goal shifts to load tolerance: being able to sustain normal daily life — work, exercise, social activity — without fatigue-driven pain onset. This involves progressively increasing exercise volume, returning to any previously avoided activities, and building postural endurance through sustained positions that previously provoked symptoms. Postural correction physiotherapy plays a role here — not in achieving a fixed ideal posture, but in reducing habitual compensatory patterns and building the body’s capacity to move through a full day without guarding.
Do’s and Don’ts
Do:
- Get a professional bra fitting from an experienced fitter — this is part of the treatment plan, not a lifestyle suggestion
- Prioritize posterior chain exercises; the back muscles need to be built, not just the front ones stretched
- Use a lumbar support cushion during prolonged sitting and break up standing with position changes every 30 to 40 minutes
- Learn the hip hinge and apply it to every forward-bending task in daily life
- Be consistent over weeks, not sessions — tissue and neuromuscular adaptation takes time
Don’t:
- Wear a compression-only sports bra for extended everyday use; it loads the thorax differently and does not distribute weight well
- Rely on chest and shoulder stretching alone — without building the posterior capacity to match, flexibility gains are unlikely to hold
- Dismiss leg-radiating, progressive, or position-independent pain as “just your posture”
- Expect visible improvement in under six weeks — this is a slow adaptation process, and impatience leads to abandoning programmes that were working
Return-to-Activity
Most women with breast-related lower back pain who engage consistently with a targeted programme can return to full activity — gym training, running, recreational sport, physically active work — within eight to twelve weeks. The indicators that signal readiness are functional rather than time-based: completing a 30-minute walk or sustained standing task without meaningful pain onset; performing a controlled hip hinge loaded to approximately 50% of body weight without discomfort; experiencing no pain increase in the 24 hours after a training session.
When Conservative Care Reaches Its Limits
If a targeted, properly executed conservative programme — correct bra fitting, posterior chain loading, postural retraining, load management — has been consistently maintained for three to four months without meaningful improvement, the clinical picture deserves reassessment.
At this point, the contribution of breast volume relative to body frame should be evaluated honestly and objectively. If macromastia is clearly present and the load-driven mechanism has not responded to all available conservative strategies, a surgical consultation is appropriate. Delaying that conversation indefinitely, while repeating variations of the same management approach, does not serve the patient.
Breast Reduction Surgery: Understanding the Evidence
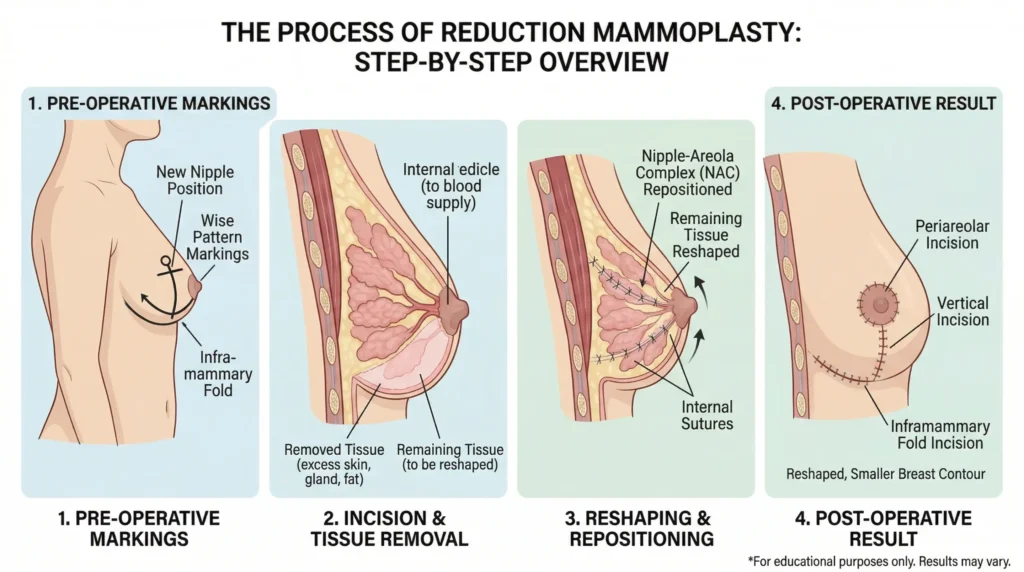
Reduction mammoplasty is among the most clinically effective elective surgical procedures when performed for the right indication. A systematic review and meta-analysis published in the European Spine Journal found that reduction mammoplasty is associated with meaningful improvement in back pain in women with large breasts, with the evidence drawn from 13 studies and a clear associative relationship identified between the surgery and reduction in back pain prevalence.
The mechanism is straightforward: removing anterior breast mass reduces the rotational torque at the lumbar spine, allows the paraspinal muscles to work at a more sustainable load, and permits spinal alignment to shift toward a less compensatory configuration. For women in whom breast volume is the dominant mechanical driver, the surgery addresses the root cause rather than its downstream consequences.
A referral for surgical assessment does not commit anyone to an operation. It opens a structured conversation about whether anatomy, symptom pattern, and prior management history together make a strong case for intervention.
Realistic Prognosis
For women who engage with targeted conservative management early, the prognosis is genuinely good. Most achieve meaningful reduction in pain frequency and severity within eight to twelve weeks, and many sustain those gains long-term through continued posterior chain training.
Women most likely to reach the limits of conservative management are those with objectively disproportionate breast volume, a long symptom history, coexisting disc or facet joint changes, or physically demanding occupations. For this group, the surgical conversation should happen earlier — not after years of incremental management that never quite resolves the underlying mechanical imbalance.
Lower back pain from large breasts is a mechanical problem with identifiable drivers and real solutions. It is not an inevitable consequence of breast size, and it does not require surgery to resolve in the majority of cases — provided the management is actually designed around the right clinical problem.
Conclusion
Lower back pain from large breasts follows a predictable biomechanical sequence: anterior breast mass shifts the center of gravity forward, forces compensatory changes across the spine, fatigues the paraspinal muscles, and overloads the lumbar joints. That mechanism is real, well-documented, and clinically manageable.
Most women benefit significantly from targeted physical therapy — centered on posterior chain strengthening, proper bra support, and postural retraining — before any surgical option is warranted. When those measures genuinely fall short, reduction mammoplasty has solid evidence behind it and deserves to be presented as a legitimate clinical pathway, not a reluctant last resort.
If this pattern of pain sounds familiar, a thorough assessment by a physical therapist (physiotherapist) who understands the breast-spine load relationship is the right first step. There is considerably more that can be done here than “improve your posture and see how it goes.”
Frequently Asked Questions
1. Can large breasts genuinely cause lower back pain, or is something else usually responsible?
Yes — breast weight can directly cause lower back pain through a well-defined biomechanical mechanism. Large breasts shift the body’s center of gravity forward, forcing compensatory spinal changes and sustained paraspinal muscle overload. That said, the diagnosis should not be made by assumption: other common causes of lower back pain in women — including sacroiliac joint dysfunction, lumbar disc involvement, and pelvic pathology — can coexist or independently account for the symptoms, and a proper clinical assessment helps distinguish between them.
2. What type of bra is most effective for reducing this kind of back pain?
An encapsulating bra — one that supports each breast separately rather than compressing both together — with wide padded shoulder straps, a stable underwire that follows the chest wall contour, and a firm band that sits horizontally across the back distributes weight most effectively across the day. A professional fitting by an experienced bra fitter is consistently worth the effort. Most women are wearing the wrong size, and an ill-fitting bra can actively worsen spinal and shoulder loading rather than reduce it.
3. Which exercises are most useful for breast-related lower back pain?
The exercises with the most consistent clinical benefit target the posterior chain — the muscles that counterbalance anterior breast load. Prone Y, T, and W drills for the lower trapezius and thoracic extensors, glute bridges for lumbopelvic stability, banded or cable rows for scapular retraction, and dead bugs for deep lumbar stabilizer activation tend to produce the most meaningful improvement. Generic abdominal exercises or chest stretches alone are insufficient; the training emphasis needs to be on building the back, not just releasing the front.
4. How do I know whether my lower back pain is from breast size or something more serious?
Pain that is bilateral, reliably worse with prolonged standing and walking, clearly better with lying down, and accompanied by upper-back or neck stiffness fits the breast-load pattern. Pain that radiates persistently down one leg, causes numbness or tingling in the feet, does not vary with any position, or occurs alongside bladder or bowel changes does not fit this pattern and requires clinical assessment. One-sided deep buttock or lower back pain provoked by stair-climbing or rolling over in bed may suggest sacroiliac joint involvement rather than breast-related loading.
5. Is breast reduction surgery medically justified for back pain?
In the appropriate clinical context, yes. When conservative management — targeted physiotherapy, correct bra support, load management — has been properly maintained without adequate relief, and breast volume relative to body frame is objectively disproportionate, reduction mammoplasty has genuine evidence supporting its role as a treatment for axial back pain. In these cases it is classified as a reconstructive procedure addressing a structural problem, not a cosmetic one, and in many healthcare systems it may qualify for coverage through a medical rather than aesthetic referral pathway.
6. How long does it take to see improvement with physical therapy?
Most women with breast-related lower back pain notice meaningful improvement after six to eight weeks of consistent, targeted exercise. Full functional benefit — being able to sustain prolonged standing, exercise, and daily activity without significant pain — typically develops over eight to twelve weeks. Improvement that plateaus early, well short of functional goals, is a signal to reassess both the exercise programme and the overall clinical picture, including whether conservative management is the right sole strategy.
7. Does losing weight reduce breast-related back pain?
It can, but not reliably for all women. Breast volume in those with primarily glandular hypertrophy is not strongly driven by body weight, and exercise-based weight loss may not meaningfully reduce breast mass in this group. Weight management can still help by improving overall spinal mechanics, strengthening the posterior chain, and reducing general load on the lumbar spine — but it should not be positioned as the primary solution when breast composition is predominantly glandular tissue.
8. Can this type of back pain develop in teenagers?
Yes. Macromastia can develop during puberty, and adolescents are not immune to breast-related postural back pain. In younger women, the spine is still adapting structurally, which makes the postural consequences of significant anterior breast load during formative years particularly relevant. Management principles are the same — posterior chain strengthening, proper bra support, movement education — though exercise prescription should be age-appropriate and supervised by a qualified physiotherapist.
Medical Disclaimer
This article is written for general informational purposes and reflects the clinical perspective of a qualified physiotherapist. It is not a substitute for a professional medical assessment, diagnosis, or individualized treatment plan. The content of this article is not intended to diagnose any condition, recommend any specific treatment, or replace the advice of your doctor or healthcare provider. If you are experiencing lower back pain, neurological symptoms, or any of the red flags described in this article, seek professional medical evaluation promptly. Do not delay seeking medical care based on information read here.
References
- Mian S, Dyson E, Ulbricht C. Reduction mammoplasty and back pain: a systematic review and meta-analysis. European Spine Journal. 2020;29(3):497–502. doi:10.1007/s00586-019-06155-2. PMID: 31606817.



