“Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.”
Yes, mild lower back pain after a chiropractic adjustment can be normal if it feels like temporary soreness or stiffness and starts settling within 24 to 48 hours. Severe pain, worsening symptoms, leg numbness, weakness, or bowel or bladder changes are not normal and need prompt medical assessment.
In other words: a brief flare is one thing; a true deterioration pattern is another.
Key Takeaways
- Mild soreness, stiffness, or a short-lived increase in pain can happen after spinal manipulation. [1]
- That kind of soreness should usually settle rather than snowball.
- Severe pain, spreading leg symptoms, saddle-area numbness, or bowel/bladder changes need prompt medical assessment. [3]
- An adjustment is not supposed to be a substitute for a full rehab plan. For low back pain, manual therapy is generally best used as part of a broader package that includes exercise and self-management. [2]
- Routine imaging is usually not needed for ordinary low back pain unless the findings would change management or there are red flags. [2]

Is lower back pain after chiropractic adjustment normal?
Yes, mild, short-term lower back pain after chiropractic adjustment can be normal. In research on spinal manipulative therapy for acute low back pain, reported harms were typically minor and transient, such as increased pain, muscle stiffness, or headache, rather than serious complications. [1]
What people often call “pain after an adjustment” is not always injury. Sometimes it is more like post-treatment soreness. A joint has been moved, surrounding muscles have reacted, tissues that were already irritated have been loaded, and the nervous system has decided to complain about it for a day or two. That can feel disappointing, but it is not automatically dangerous.
The problem is that the word normal gets abused. Normal does not mean “ignore anything.” It means the response fits a predictable, short-lived soreness pattern and then begins to settle.
Why your back may hurt after an adjustment
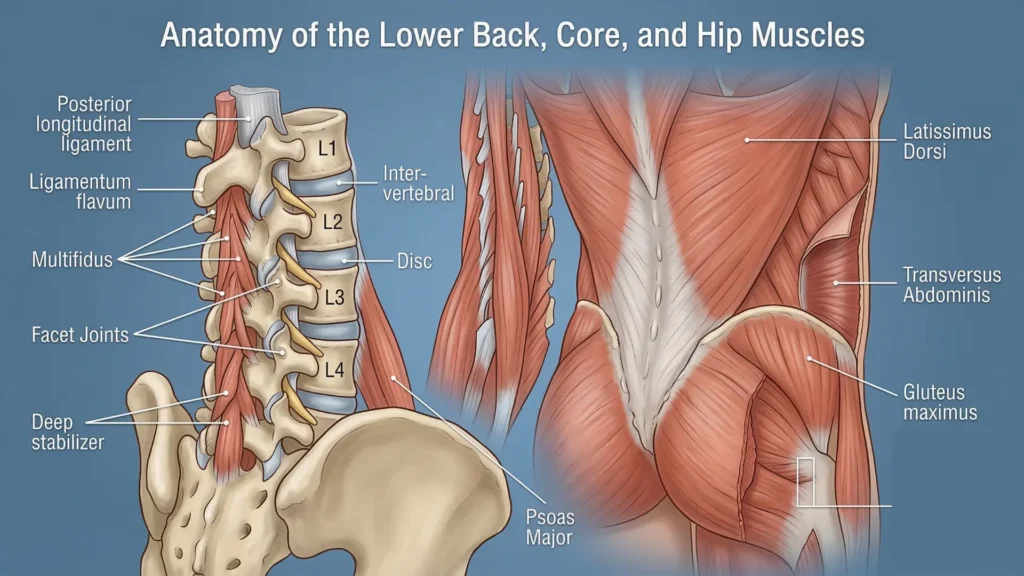
A chiropractic adjustment is a mechanical input. Your low back is not just vertebrae stacked like bricks. It is a system of discs, facet joints, ligaments, deep stabilizers, larger trunk muscles, hip muscles, and a nervous system that constantly decides what feels safe and what does not.
Several things may create soreness afterward:
1. Muscle guarding or reactive spasm
If the area was already irritated, the surrounding muscles may tighten afterward. This is common when the back has been sensitive for days or weeks before treatment.
2. A previously irritable joint or disc got stressed
An adjustment may be tolerated well by one person and poorly by another. If you already had a disc-related flare, a facet irritation, or an angry sacroiliac region, even a technically competent treatment can temporarily stir symptoms up.
3. Your system was sensitized before the visit
Many backs are already “hot” before treatment. The adjustment becomes the event people blame, but the tissue and nervous system were already primed to react.
4. The treatment was not the right match for that stage
Manual therapy can help some people, but it is not universally the right tool for every presentation, every direction of pain, or every level of irritability. NICE recommends manual therapy only as part of a treatment package that includes exercise, not as a stand-alone long-term strategy. [2]
What soreness is more likely to be expected?
A post-adjustment soreness pattern is more likely to be expected when the pain is:
- dull, achy, or stiff rather than sharp and escalating
- local to the low back or upper buttock
- worse for a few hours or up to a day or two, then gradually easing
- not associated with new numbness, clear weakness, or loss of control in the leg
- improved by walking gently, changing position, heat, or time
This can feel similar to how your body reacts after returning to the gym and deciding, the next morning, to send a formal complaint.
When lower back pain after chiropractic adjustment is more concerning
Lower back pain after chiropractic adjustment is not something to brush off when the pattern clearly moves beyond ordinary soreness.
Seek prompt medical attention if you develop any of the following:
- pain that is severe and not settling
- pain that starts radiating strongly down the leg
- new weakness in the leg or foot
- numbness in the buttock, groin, genitals, or “saddle” area
- new trouble starting urination, loss of bladder or bowel control, or loss of sensation when passing urine or stool
- unexplained fever, night pain, or a markedly different pain pattern than usual [3]
Those features do not automatically mean the adjustment caused a serious injury. But they do mean the situation should be assessed properly rather than explained away with, “It’s just settling.”
Do you need an MRI or X-ray?
Usually, not right away.
For most uncomplicated low back pain episodes, guidelines do not recommend routine imaging in non-specialist settings. Imaging is generally considered when there are red flags, significant neurologic findings, or when the result is likely to change management. [2] If you want to which type of changes you can see in MRI report read Crucial Understanding: Modic Changes on MRI & What They Mean for Your Back Pain.
That matters because many people panic after a painful treatment and rush to get a scan. The scan often shows age-related changes that were already there, which can increase fear without improving the plan. The better question is not “Can I see something on imaging?” It is “Would imaging change what needs to happen next?”
Common symptom patterns and what they may suggest
Mostly local soreness
This more often points toward a temporary soft-tissue or joint irritation pattern.
Back pain plus buttock pain
This may still be mechanical and local, but it deserves a closer look at the facet joints, sacroiliac region, gluteal loading, and hip movement.
Back pain plus leg pain, tingling, or numbness
This raises more concern for nerve-root irritation, especially if the symptoms travel below the knee or are accompanied by weakness.
Pain that was mild before treatment and clearly worse after
This does not prove harm, but it does justify reassessment. The clinical question becomes: is this a short irritability flare, or did the treatment direction not suit the problem?
Myths that confuse people after an adjustment
Myth 1: “If I hurt afterward, something must have been put out of place.”
Not necessarily. Most post-treatment soreness is better understood as a tissue and nervous-system response, not a vertebra suddenly wandering off like it missed its train.
Myth 2: “If it cracked loudly, it must have worked.”
The sound tells you gas changed pressure in a joint. It does not tell you how much long-term benefit you got.
Myth 3: “If it helped once, I just need more adjustments forever.”
That is a weak long-term strategy for most back problems. Manual therapy may reduce pain temporarily, but durable improvement usually comes from graded movement, load tolerance, strength, confidence, and behavior change. [2]
This is where many people get stuck: they keep comparing one passive treatment against another, when the real issue is that both may offer only temporary symptom relief if the underlying movement and loading problem is never addressed. If you want a broader breakdown of this, read our article on chiropractor vs massage for lower back pain, which explains why both are often temporary and what actually creates longer-term improvement.
From the Clinic: Dr. Arora’s Expert Insight
One very important point patients need to understand is that chiropractic adjustment is not suitable for everyone. There are specific cases where this type of treatment may help, but in many lower back conditions, it may also increase pain if used in the wrong person or at the wrong stage. Before you lie down on the table, ask your chiropractor clearly: “Am I actually an appropriate candidate for this type of adjustment?”
For example, if you have moderate to severe spinal degeneration, this kind of forceful treatment may aggravate symptoms, increase tissue irritation, and potentially worsen the problem rather than help it. In many cases, the person is not reacting to one adjustment in isolation. They are reacting to an already irritable back with poor load tolerance, limited hip contribution, too much protective bracing, and not enough capacity.
The mistake is assuming the only question is, “Was the adjustment good or bad?” In real life, the better question is, “What was my back actually capable of tolerating that day?” I often see people sit all week, get treated, feel slightly looser, and then immediately test that improvement by bending poorly, driving long hours, lifting awkwardly, or returning to gym loads their body was not ready for. When the flare follows, the treatment gets blamed entirely.
What to do in the next 24 to 72 hours
If the pain feels like ordinary post-treatment soreness, the goal is not full bed rest. It is relative calm.
Helpful steps
- Take short, easy walks.
- Change position regularly instead of sitting in one posture for hours.
- Use heat if it relaxes the area; some people prefer a brief trial of ice.
- Sleep in the least provocative position, often with a pillow support if needed.
- Avoid testing the pain every 20 minutes by repeatedly bending to “see if it’s gone.”
- Use medication only if it is medically appropriate for you and consistent with advice from your clinician.
Avoid for the moment

- heavy lifting
- repeated end-range bending and twisting
- max-effort gym work
- long static sitting if it clearly aggravates symptoms
- another treatment session simply because you feel panicked, not because the pattern was reassessed
For low back pain more broadly, advice to stay active and self-manage is supported in guidance, while prolonged rest is not the preferred approach. [2][3]
A sensible rehab progression
Phase 1: Settle the flare
The first target is symptom control and movement confidence.
Useful options may include:
- short walks
- comfortable pelvic tilting or gentle lumbar motion
- breathing with abdominal relaxation rather than constant bracing
- supported sit-to-stand practice
- finding a less provocative bend pattern
Phase 2: Restore movement options
Once symptoms are calming, work on:
- hip hinge mechanics
- gentle trunk control
- glute contribution
- reducing fear of normal movement
This stage is about teaching the body that everyday motion is not a threat.
Phase 3: Rebuild load tolerance
Now the focus shifts to:
- carries
- step-ups or split-squat patterns
- bridge variations
- anti-rotation trunk work
- progressive return to gym or sport tasks
That progression matters. A back that is only pain-calmed but not load-trained is often one awkward grocery bag away from another dramatic relapse.
Do’s and don’ts
Do
- monitor the overall trend, not every single twinge
- keep moving within reason
- ask whether symptoms are becoming more local and less intense
- get reassessed if symptoms are clearly worsening or changing character
Don’t
- assume every crack or adjustment is corrective
- lie in bed for days unless a clinician specifically advised it
- push through sharp radiating pain to prove toughness
- let anyone dismiss new neurologic symptoms as routine soreness
When conservative care is failing
You need a more careful review if:
- pain is not trending down after several days
- pain is repeatedly flared by simple daily tasks
- leg symptoms are appearing or worsening
- you cannot walk, sleep, or function normally
- you feel stuck in a cycle of short-term relief and recurrent flare-ups
At that point, the plan may need a different diagnosis, a different loading strategy, medication review, imaging if indicated, or referral to the right specialist.
When surgery may be considered
Surgery is not a treatment for ordinary post-adjustment soreness.
It may enter the discussion when there is a clearly defined structural problem that matches the symptoms and examination, especially with significant neurologic deficit, persistent disabling radicular pain that does not improve with appropriate conservative care, or emergency patterns such as cauda equina syndrome. [3]
Conclusion
Lower back pain after chiropractic adjustment can be normal when it is mild, local, and short-lived. What matters is the pattern. If the pain is settling, it may simply be transient post-treatment soreness. If it is escalating, spreading, or paired with numbness, weakness, or bowel or bladder symptoms, stop guessing and get assessed.
The safest frame is simple: do not panic over a brief ache, but do not normalize a clear red-flag pattern either.
FAQs
1. Is it normal to feel worse the day after a chiropractic adjustment?
Yes, a mild temporary increase in soreness or stiffness can happen the next day. That is more reassuring when it stays local, is manageable, and begins settling rather than intensifying. [1]
2. How long should lower back pain after chiropractic adjustment last?
It should usually be brief. If it is ordinary post-treatment soreness, it should trend in the right direction over the next day or two rather than continue escalating.
3. Can a chiropractic adjustment cause sciatica-like pain?
It can temporarily aggravate an already irritable nerve-related pattern in some people. New leg pain, tingling, numbness, or weakness deserves reassessment instead of being written off as routine soreness.
4. Should I use ice or heat after an adjustment?
Use whichever clearly calms the area. Heat often helps stiffness and guarding, while ice may help some people if the area feels sharply irritated.
5. Should I rest completely after an adjustment?
No, complete rest is usually not the best response. Most people do better with gentle movement, position changes, and a gradual return to normal activity. [2][3]
6. When do I need imaging after an adjustment?
You usually do not need imaging just because you are sore afterward. Imaging is more relevant when there are red flags, important neurologic findings, or when the result would change management. [2]
7. Can I go back to the gym after an adjustment flare?
Yes, but not by pretending nothing happened. Return once symptoms are calming, then restart with lighter loads, cleaner hinge mechanics, and less end-range aggression.
8. Should I get adjusted again if the first one made me worse?
Not automatically. First decide whether this was simple short-term soreness or a sign that the treatment choice, force, timing, or diagnosis needs to be reconsidered.
Medical Disclaimer
This article is for general educational purposes only and is not a diagnosis or a substitute for in-person medical care. If you have severe or worsening pain, new weakness, numbness, saddle-area symptoms, fever, or bowel or bladder changes, seek urgent medical assessment.
References
- Paige NM, Miake-Lye IM, Booth MS, et al. Association of Spinal Manipulative Therapy With Clinical Benefit and Harm for Acute Low Back Pain: Systematic Review and Meta-analysis. JAMA. 2017;317(14):1451-1460. doi:10.1001/jama.2017.3086.
- National Institute for Health and Care Excellence (NICE). Low back pain and sciatica in over 16s: assessment and management (NG59). Guidance and recommendations.
- MedlinePlus / NHS sources on urgent low back pain warning signs and cauda equina symptoms.



