“Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.”
Deadlift and lower back pain is one of those topics that gets ruined by extremes. One camp says, “Your form was bad, so you injured your spine.” The other says, “Relax, everyone’s back rounds, just keep lifting.” Neither is especially helpful when your back is barking every time the bar leaves the floor.
As a Physical Therapist (physiotherapist), I usually find that the painful rep was not the whole story. The real story is often a stack of smaller decisions: too much load for current tolerance, rushed setup, poor bracing, bar drift, fatigue, or trying to force a deadlift style your body does not currently own. The deadlift itself is not automatically the villain. More often, it is the audit.
This article explains why Deadlift and Lower Back Pain often show up together, how to tell a manageable overload from something that needs medical attention, and which nine form fixes usually make the biggest difference.
Key Takeaways
- Lower back pain during deadlifts is often a load-management and execution problem, not proof that you have “damaged” your back.
- A slightly flexed lumbar spine is not automatically dangerous. The stronger question is whether the position is controlled, repeatable, and appropriate for the load. A systematic review found low-quality evidence that greater lumbar flexion during lifting was not a clear risk factor for low back pain onset or persistence.
- Routine imaging is usually not needed for ordinary low back pain after lifting unless there are red flags or the result would change management. NICE advises against routinely offering imaging in non-specialist settings for low back pain and recommends imaging in specialist care only if it is likely to change management.
- Most lifters do better with temporary load reduction, cleaner mechanics, and a graded return than with either complete rest or stubbornly training through worsening symptoms. NICE also advises tailored self-management and encouragement to continue normal activities.
- Severe pain, spreading leg pain, numbness, weakness, bowel or bladder changes, fever, or major trauma are not “fix your form and see” situations. NICE specifically recommends excluding serious causes such as cancer, infection, trauma, or inflammatory disease when symptoms suggest them.

Why does my lower back hurt when I deadlift?
Lower back pain during deadlifts usually happens when the lumbar area takes more load than it can currently tolerate, often because of poor bracing, bar drift, reduced hip contribution, fatigue, or using more weight than your current mechanics can control. That does not automatically mean you have seriously injured your back.
Deadlift and Lower Back Pain: what is usually going wrong?
The deadlift is a force-transfer exercise. The legs push, the hips extend, the trunk stiffens, and the bar travels close to the body. When that sequence is clean, the load is shared. When it is messy, the lower back often becomes the unpaid intern doing everyone else’s job.
Three things usually decide whether the back stays calm or gets grumpy:
- Where the load is
If the bar drifts forward, the back works harder. - How well the trunk is organized
If you lose pressure, the spine has to manage motion and load at the same time. - Whether the hips are actually contributing
If the hips stop producing force, the lumbar area often picks up the slack.
This is why two lifters can use the same exercise and get very different outcomes. One person is expressing strength. The other is negotiating with physics.
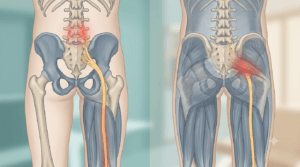
What your lower back is supposed to do in a deadlift
Your lower back is not supposed to be the prime mover in a deadlift. Its main role is to provide enough stiffness and positional control for force to pass from the floor, through the legs and hips, into the bar.
That does not mean your spine must look like a textbook drawing. Real lifters are not anatomy posters. It does mean the position should be controlled rather than collapsing, and consistent rather than changing rep to rep under fatigue. That distinction matters more than social-media arguments about whether the spine is “perfectly neutral.” The available review evidence does not support the simplistic rule that more lumbar flexion during lifting automatically predicts low back pain.
What the timing of pain often tells you
This is where articles often become generic. Timing matters.
Pain right off the floor
This often points to one of four problems: the bar starts too far forward, you yank instead of wedging in, you lose brace early, or the hips shoot up before the bar really moves. In clinic and in the gym, this is one of the most common patterns I see in lifters who say, “My setup looks fine on video,” but the first inch of the pull tells the real story.
Pain around the knee
This often happens when the bar has drifted away and you are now dragging a longer lever arm up the body. It can also happen when the lats never really engaged, so the bar path became more “out and around” than “up and close.”
Pain at lockout
This is a classic one. Many lifters finish by leaning back instead of standing tall. They thrust the hips through, shove the ribs up, and dump compression into the lower back. Then they blame the floor break, when the actual insult happened at the top.
Pain mostly the next day
This pattern is often less alarming and more consistent with overload, tissue irritability, or a volume jump that exceeded tolerance. It still deserves respect, but it is not the same thing as sharp, spreading pain during the lift.
9 form fixes that usually help

1) Start with the bar where the lift can actually work
If the bar begins too far in front of midfoot, the lower back starts the rep at a mechanical disadvantage.
Fix: Set the bar over the midfoot before you bend down. Then leave it there. Do not nudge it forward while taking your grip, and do not let your setup turn into a small treasure hunt where the bar ends up farther away each second.
2) Stop trying to squat your deadlift off the floor
Many lifters drop the hips too low because it feels safer. The result is often the opposite: the hips pop up first, the back angle changes, and the lower back takes a messy hit before the plates are even moving cleanly.
Fix: Let your hips sit high enough for the hamstrings and glutes to load. If the first thing your hips do is shoot upward, your start position was probably too low.
3) Build pressure before the pull, not during it
A deadlift should not begin with surprise. If the bar is moving before your trunk is organized, the spine is managing load with a half-finished brace.
Fix: Take your breath, expand into the lower ribcage and abdomen, lock the trunk, engage the lats, then pull. A good brace feels like the rep is already “on” before the bar leaves the floor.
4) Keep the bar close enough that your back is not chasing it
When the bar drifts forward, the lower back pays. This is one of the most reliable reasons a set that felt fine at rep one becomes ugly by rep four.
Fix: Think “bar up the legs,” not “bar out in front of me.” The lats help here. If you do not feel them, the bar often wanders and your back gets promoted to chief compensator.
5) Wedge in; do not yank
A violent jerk off the floor is a good way to turn a manageable lift into a cranky back.
Fix: Pull the slack out first. Feel the body connect to the bar. Let the plates break from tension, not from panic. This single change often helps lifters who swear they “randomly” hurt their back on otherwise routine weights.
6) Do not confuse “neutral” with “overarched”
Some lifters avoid rounding by aggressively arching the lower back and flaring the ribs. That can feel strong for about three seconds, then become irritating under load.
Fix: Aim for a stacked torso, not a theatrical chest-up posture. The evidence does not support a blanket rule that more lumbar flexion during lifting automatically separates people with and without low back pain, so the goal is organized loading, not a rigid aesthetic posture contest.
7) Let the hips hinge instead of asking the back to do hip work
A deadlift is not just “bend down and stand up.” The hips need to move back and then extend powerfully. When they do not, the back often becomes the main engine instead of the transmission tower.
Fix: If you struggle to feel hamstrings and glutes but feel everything in the lower back, practice the hinge separately with Romanian deadlifts, dowel hip hinges, kettlebell deadlifts from blocks, or cable pull-throughs.
8) Respect the rep where your form quietly changes
Back pain in deadlifts often shows up on the rep that looks only slightly different to the eye but very different to the body. The brace softens. The bar drifts. The lockout turns into a lean-back. The spreadsheet still says “5,” so people do rep five and then act surprised that anatomy had opinions.
Fix: End the set when the movement stops looking like the version you meant to train. This is not weakness. It is load management.
9) Lock out with the glutes, not with a backward lean
A good lockout is tall and strong. A bad lockout looks like someone trying to impress a chiropractor in a parking lot.
Fix: Finish by squeezing the glutes and bringing the ribs over the pelvis. Stand tall. Do not hinge backward at the end of the rep and call it powerlifting.
Is it soreness, overload, or something more serious?
The answer depends on the pattern, not just the intensity.
More consistent with a manageable mechanical flare-up
- dull or local ache in the low back
- stiffness the next morning
- discomfort linked to loading, bending, or getting out of a chair
- no numbness, tingling, or spreading leg pain
- symptoms that settle when load is reduced
More concerning
- sharp pain that stopped the lift immediately
- pain shooting below the knee
- progressive numbness, weakness, or loss of coordination
- severe pain that is escalating rather than easing over the next 24 to 48 hours
- bowel or bladder changes
- pain plus fever, unexplained weight loss, major trauma, or significant night pain
NICE recommends thinking about alternative diagnoses and excluding serious causes such as cancer, infection, trauma, or inflammatory disease when the presentation suggests them.
When imaging is and is not needed
A scan is not a trophy for having back pain. Most lifters with ordinary mechanical low back pain after deadlifting do not need immediate imaging.
NICE advises against routinely offering imaging in a non-specialist setting for low back pain with or without sciatica, and says imaging in specialist care should be considered only if it is likely to change management.
That matters because many imaging findings can exist in people who are functioning reasonably well. If the scan result would not change what you do, it often adds more noise than value.
Imaging becomes more relevant when:
- serious pathology is suspected
- there is meaningful or progressive neurological deficit
- symptoms are persistent and not behaving like a routine mechanical flare-up
- a specialist decision is being considered and the result would alter treatment
Myths that keep lifters stuck
“If my back hurt, my form must have been terrible.”
Not necessarily. Sometimes the form was acceptable, but the load, fatigue, or recent training context was not.
“Any rounding means injury.”
Too simplistic. The better question is whether the position is controlled and appropriate for the load. The best available review on this specific issue did not find clear evidence that greater lumbar flexion during lifting is a risk factor for low back pain onset or persistence.
“I need complete rest until it settles.”
Usually not. NICE recommends advice that supports self-management and encourages continuation of normal activities as able, rather than unnecessary shutdown.
“I should just push through it so I don’t get weak.”
Also not wise. There is a large difference between tolerable loading and repeatedly rehearsing the exact pattern that is irritating the back.
From the Clinic: Dr. Arora’s Expert Insight
People judge the deadlift only by what it looks like from the side on their best rep with the max weight they can lift once. The body, unfortunately, does not grade your lift based on your prettiest angle.
What actually predicts trouble more often in real life is inconsistency. The warm-up set looks organized. The first work set looks acceptable. Then fatigue arrives, and small leaks appear everywhere: the brace gets softer, the bar drifts two centimeters forward, the lockout becomes a lean-back, and the hips stop contributing at the exact moment the lifter starts trying harder. That combination is far more clinically useful than obsessing over whether the lumbar spine was perfectly neutral to the degree.
Another thing people misunderstand is pain location. If someone tells me, “It catches right as I break from the floor,” I think about setup, bar distance, wedge, and brace timing. If they say, “It pinches more at the top,” I think about overextension, rib flare, and a poor lockout strategy. If they say, “The set feels fine but I am wrecked the next morning,” I think about tolerance, volume, recovery, and how recently they increased load. Generic advice misses these distinctions, which is why generic advice often fails.
What usually works better is much less dramatic than social media makes it sound: reduce the threat, clean up the setup, lower the load temporarily, restore a reliable hinge, and then build tolerance back in stages. Most lifters do not need a funeral for the deadlift. They need a better conversation with it.
What to do in the next 24 to 72 hours
If you do not have red flags, the short-term goal is to calm the back down without teaching it that movement is dangerous.
A reasonable early plan is:
- stop painful heavy pulling for now
- keep walking and moving normally as tolerated
- use relative rest instead of bed rest
- avoid “testing it” every day with the same painful movement
- train around it if you can do so without aggravating symptoms
- reintroduce hinge work at a level your body can organize
That approach fits current low back pain guidance. NICE recommends tailored advice and information to support self-management, plus encouragement to continue normal activities. It also recommends considering exercise based on the person’s needs and capabilities.
Your next gym session: what to actually change
This is the part many readers want and most articles undercook.
For the next session, do not ask, “Can I deadlift exactly the same way and see if it hurts less?” Ask, “What version can I do cleanly today?”
A useful reset looks like this:
- reduce the load meaningfully
- perform dead-stop reps instead of touch-and-go
- shorten the set length
- use more rest between sets
- film one working set
- stop at the first clear technical drift
- consider raising the bar slightly or using blocks if the floor position is the trigger
If straight-bar deadlifts still feel provocative, switch temporarily to a friendlier hinge pattern such as Romanian deadlifts, block pulls, or trap-bar work if available. The goal is not to win an argument with the barbell. The goal is to reload the pattern without re-irritating the back.
A practical return-to-deadlift progression
Phase 1: settle the flare
Goal: reduce irritability while keeping confidence in movement.
Options:
- walking
- bodyweight hip bridges
- unloaded or lightly loaded hinge drills
- trunk bracing practice
- gentle posterior-chain work that does not provoke symptoms
Phase 2: rebuild the hinge
Goal: restore a clean movement pattern.
Options:
- kettlebell deadlifts from blocks
- Romanian deadlifts
- dowel hinge drills
- cable pull-throughs
- paused light deadlifts if tolerated
Phase 3: reload with rules
Goal: build tolerance, not bravado.
Rules:
- use lower reps per set
- leave reps in reserve
- stop if the rep shape changes
- keep the bar close
- preserve the same brace quality from rep one to the last rep
Phase 4: return to normal programming
Goal: resume ordinary training without repeating the same mistake.
Only push load when:
- pain is stable or absent
- next-day symptoms are acceptable
- the setup is repeatable
- the lockout is clean
- you are no longer negotiating every rep with the lower back
Do’s and don’ts
Do
- warm up gradually
- respect fatigue
- treat setup as part of the lift
- keep the bar close
- use video to check trends, not to worship one freeze-frame
- progress load gradually
Do not
- max out to “prove it’s fixed”
- aggressively arch to avoid mild flexion
- keep training through spreading leg symptoms
- confuse stubbornness with resilience
- ignore sleep, recent workload, or recovery debt
When conservative care is not enough
Get assessed if:
- symptoms are not improving over the next couple of weeks
- pain keeps returning every time you reload
- you cannot find a tolerable progression
- symptoms are spreading into the leg
- normal daily activities are still clearly limited
NICE recommends stratified management, simpler support for those likely to recover quickly, and more complex support for people at higher risk of poor outcome or those who need exercise with or without additional therapy.
When surgery may be considered
For ordinary deadlift-related mechanical low back pain, surgery is usually nowhere near the first conversation.
The more relevant surgical discussion is typically around persistent sciatica with matching radiological findings after non-surgical care has not improved pain or function. NICE recommends considering spinal decompression for sciatica in that specific context, while also advising against spinal fusion for low back pain unless as part of a randomized controlled trial.
That is another reason not to dramatize every painful deadlift into a surgical storyline.
Outlook: can you deadlift again?
In many cases, yes.
If your symptoms are local, mechanical, and improving, a return to deadlifting is often realistic. The back usually tolerates what it is prepared for. The goal is not just pain reduction; it is building a version of the deadlift your body can trust again.
What usually delays recovery is not one imperfect rep. It is repeatedly provoking the same pattern while calling it determination.
Conclusion
Deadlift and Lower Back Pain does not automatically mean your spine is damaged or that deadlifts are off-limits forever. More often, it means the lift stopped being shared well: the bar drifted, the brace leaked, the hips went quiet, fatigue took over, or the load got ahead of your current capacity.
The best response is neither panic nor denial. Clean up the setup, reduce the load temporarily, match the variation to your current tolerance, and rebuild in stages. If symptoms are severe, spreading, or neurological, get assessed. If they are local and settling, the deadlift is usually something you can earn back.
FAQs
1. Is lower back soreness after deadlifts normal?
Yes, mild local soreness can be normal, especially after a load jump, higher volume, or a change in exercise variation. What is less reassuring is sharp pain, worsening pain, or symptoms that spread into the leg.
2. Why does my lower back hurt more at lockout than off the floor?
That often happens when you finish by leaning backward instead of standing tall through the glutes. Overextension at the top can irritate the lower back even when the floor break felt fine.
3. Should I stop deadlifting completely if my back hurts?
Not always. Many lifters improve with temporary load reduction, a cleaner setup, and a graded return. Stop heavy painful pulling, but do not assume the deadlift is banned forever unless your symptoms or examination suggest something more serious.
4. Is a rounded back always dangerous in the deadlift?
No. A controlled amount of lumbar flexion is not automatically the same as an injury. The review evidence on lifting posture does not support the blanket claim that greater lumbar flexion during lifting clearly predicts low back pain.
5. When should I get a scan for back pain after deadlifting?
Usually when serious pathology is suspected, there is meaningful neurological loss, or the result would change management. NICE advises against routine imaging in non-specialist settings for ordinary low back pain.
6. Is complete rest the best way to calm a deadlift-related back flare?
Usually no. Current guidance favors tailored self-management and continuing normal activities as tolerated rather than unnecessary inactivity.
7. Can I still train legs if deadlifts are irritating my back?
Often yes. You may need to choose exercises and loading strategies that do not reproduce the same painful pattern while the back settles and the hinge is rebuilt.
Medical Disclaimer
This article is for educational purposes only and does not replace personal medical evaluation, diagnosis, or treatment. Seek prompt medical care if you have severe or worsening pain, bowel or bladder changes, saddle numbness, progressive weakness, fever, major trauma, unexplained weight loss, or persistent symptoms that are not improving.
References
- Saraceni N, Kent P, Ng L, Campbell A, Straker L, O’Sullivan P. To Flex or Not to Flex? Is There a Relationship Between Lumbar Spine Flexion During Lifting and Low Back Pain? A Systematic Review With Meta-analysis. J Orthop Sports Phys Ther. 2020;50(3):121-130. doi:10.2519/jospt.2020.9218. PubMed:
- National Institute for Health and Care Excellence (NICE). Low back pain and sciatica in over 16s: assessment and management (NG59). Published November 30, 2016. Updated December 11, 2020. Recommendations: