“Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.”
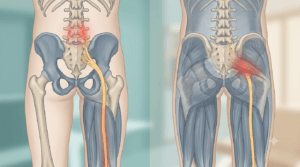
Pain near your lower back dimples is almost never caused by the dimples themselves. The discomfort usually comes from nearby structures — most commonly the sacroiliac (SI) joints, the posterior pelvic ligaments, the lower lumbar facet joints, or the muscles and fascia that cross that region. Understanding which tissue is irritated — and why — is the first step toward getting better.
If you have pain around the small indentations on either side of your lower spine, it is natural to wonder whether the dimples themselves are the problem. In most cases, lower back dimples pain is not caused by the dimples as skin features. The pain usually comes from nearby structures such as the sacroiliac (SI) joints, the ligaments that support the back of the pelvis, the lower lumbar facet joints, or the muscles and fascia that cross that region.
A 2023 observational study reported in its results that there was no statistically significant relationship between the presence of dimples of Venus and low back pain, although the main focus of the paper was anatomical associations such as pelvic incidence and facet orientation.
As a physical therapist (PT), I treat this as a regional load-transfer problem first and a “dimple problem” second. The real question is usually not “Are my dimples abnormal?” It is “Which tissue around this area is getting irritated by bending, twisting, standing, sitting, carrying, rolling in bed, walking, running, or a sudden spike in activity?” NICE guideline NG59 also supports this general approach: clinical assessment first, advice to self-manage and continue normal activities as tolerated, and selective use of imaging rather than rushing straight to scans for every episode of mechanical back pain.

Key Takeaways
- Pain near lower back dimples usually comes from structures underneath or around the dimples, not from the dimples themselves.
- Common mechanical causes include SI joint irritation, posterior pelvic ligament strain, lower lumbar facet irritation, and myofascial overload.
- Pain location alone cannot confirm the exact source; movement pattern, aggravating activities, and associated symptoms matter more.
- Urgent red flags include bowel or bladder changes, saddle numbness, fever, major trauma, progressive leg weakness, or unexplained systemic illness.
- Early management usually works best with relative activity, load modification, short walks, and targeted rehab rather than complete bed rest.
- Imaging is often unnecessary early on unless red flags are present or the result would clearly change management.
Lower Back Dimples Pain: Anatomy, Causes, and Symptom Patterns
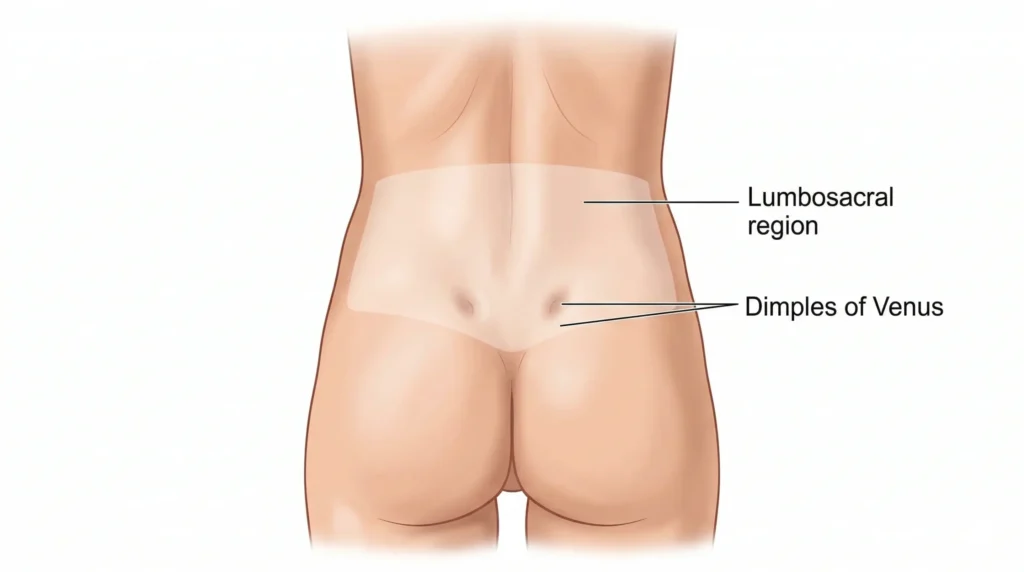
What are lower back dimples?
Lower back dimples are commonly called dimples of Venus. They are visible indentations near the back of the pelvis, close to the lumbosacral region and superficial to the area of the SI joints. Clinically, they are useful as landmarks, but that does not mean they are the injured tissue. When people point to pain “in the dimples,” they are often indicating a pain zone that overlaps with the SI region, the upper gluteal fascia, the posterior pelvic ligaments, the lower lumbar facets, and the paraspinal muscles.
Why pain often localizes around the dimples
This area is where force is transferred between the trunk and the pelvis. Every time you bend to pick something up, step into a long stride, twist while carrying a load, stand on one leg, or change position in bed, the lower lumbar spine and pelvis have to share load well. If one area becomes stiff and another area becomes overloaded, pain can localize near the dimples even when the dimples themselves are perfectly normal.
That is why people with very different problems can point to almost the same spot. One person may have a sensitive SI region. Another may have facet irritation. A third may simply have overloaded the muscles and fascia with a sudden burst of lifting, cleaning, gym work, or prolonged sitting.
Common causes of pain near lower back dimples
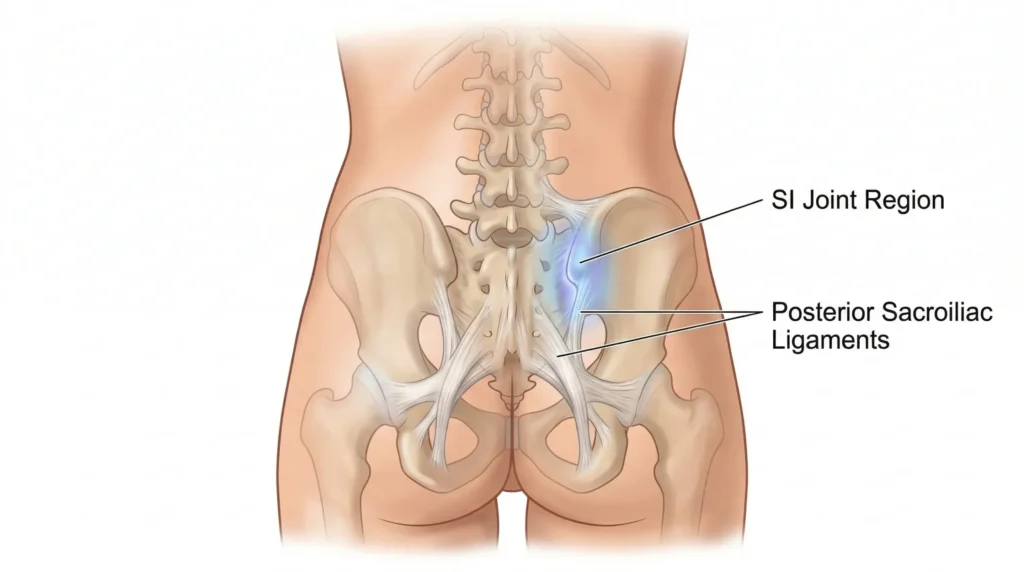
Sacroiliac joint irritation
The SI joint region is one of the most common reasons people feel pain close to the lower back dimples, especially if the pain sits just off the midline and toward the top of the buttock. It may be aggravated by single-leg loading, stairs, uphill walking, rolling in bed, getting out of a car, asymmetrical standing, pregnancy-related load changes, or a sudden increase in running or training volume.
Posterior pelvic ligament strain
The ligaments around the back of the pelvis can become sensitive after awkward lifting, repeated bending and twisting, a slip, a stumble, or a flare-up after prolonged guarding. This type of pain is often local, nagging, and mechanically irritable. People sometimes describe it as a pinpoint ache or a deep bruise-like sensation around one dimple.
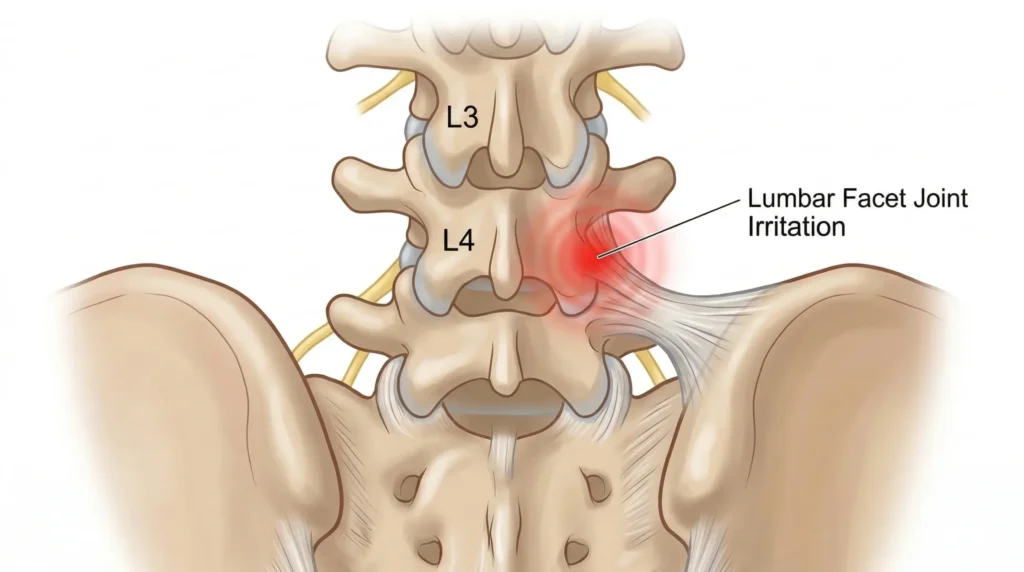
Lower lumbar facet irritation
Facet-related pain often sits a little above the dimples or overlaps with them. It may feel worse when standing upright for long periods, leaning backward, or rotating. Many people describe a pinching, jammed, or stuck feeling rather than a broad muscular ache.
Myofascial pain and trigger points
The erector spinae, multifidus, quadratus lumborum, and upper gluteal tissues can all refer pain into the dimple region. This is common after a sudden gym return, prolonged desk work, repetitive household tasks, long drives, or deconditioning. The area may feel broad, tight, and tender to touch rather than sharply localized.
Referred lumbar pain
Not every pain near the lower back dimples is an SI problem. Disc-related pain, movement-sensitive nonspecific low back pain, and other lumbar sources can all refer discomfort into the same area. This is one reason self-diagnosis based only on location is unreliable.
Less common but important causes
Sometimes pain in this region is not primarily mechanical. Inflammatory sacroiliac conditions, stress injury, fracture, infection, kidney-related pain, and some abdominal or gynecologic problems can mimic musculoskeletal pain around the dimples. These are much less common than simple mechanical pain, but they matter because the treatment path is different.
Symptom patterns: what it could be and what it may not be
| Pattern | What it may suggest | What makes me think more broadly |
|---|---|---|
| One-sided pain near the dimple or top of the buttock, worse with rolling, stairs, long stride, or single-leg stance | SI region irritation or posterior pelvic ligament sensitivity | Fever, abdominal symptoms, major trauma, or pain that does not change with movement |
| Pain slightly above the dimples, worse with standing tall, extension, or repeated rotation | Lower lumbar facet irritation | Strong nerve symptoms below the knee or clear systemic illness |
| Broad ache with local tenderness and stiffness after activity or sitting | Muscular or fascial overload | Severe night pain, unexplained weight loss, or neurological decline |
| Pain with coughing, sneezing, flexion sensitivity, or leg referral | Referred lumbar pain or disc-related irritation | Purely local soreness with no movement-related pattern |
| Morning pain with prolonged stiffness, alternating buttock pain, and slow warm-up | Inflammatory back pain or inflammatory SI involvement | Pain that is clearly dose-dependent, settles quickly with simple load reduction, and lacks persistent morning stiffness or systemic features |
No single home test can diagnose this perfectly. The pattern becomes clearer when you combine the story, pain behavior, physical examination, and the way symptoms respond over several days.
Red flags: when to seek urgent care
Seek urgent care or emergency assessment if you have:
- new bowel or bladder dysfunction, especially urinary retention
- saddle numbness
- progressive leg weakness
- fever, chills, or feeling unwell with significant back pain
- major trauma
- unexplained weight loss or known cancer history with new back pain
- severe unrelenting night pain or rapidly worsening symptoms
These features raise concern for causes that should not be managed like routine mechanical low back pain.
When imaging is needed, and what imaging can and cannot tell you
Most people with recent mechanical pain around the lower back dimples do not need immediate X-rays or an MRI. NICE guideline NG59 advises against routinely offering imaging in a non-specialist setting for low back pain with or without sciatica, and recommends considering imaging mainly when the result is likely to change management.
Imaging can help look for fracture, infection, inflammatory disease, significant structural pathology, or nerve compression when the clinical picture supports it. What it cannot do is guarantee that every age-related change seen on a scan is the true pain generator. Many people have imaging findings that look dramatic but are not the main reason their current flare is hurting.
Myths vs Facts
Myth: The dimples themselves are damaged.
Fact: Usually, no. The painful tissue is more often a joint, ligament, muscle, fascia, or referred lumbar source near the dimples.
Myth: Pain near back dimples always means SI joint dysfunction.
Fact: Not always. SI irritation is common in this area, but facets, muscles, fascia, and referred lumbar pain can feel very similar.
Myth: If the pain is one-sided, it must be serious.
Fact: One-sided mechanical pain is very common. It becomes more concerning when it is paired with fever, trauma, progressive weakness, or other red flags.
Myth: You need a scan right away.
Fact: Usually not. As reflected in NICE guideline NG59, many episodes improve with good assessment, symptom modification, and graded rehab without immediate imaging.
Myth: The best treatment is complete rest.
Fact: Usually not. NICE guideline NG59 supports self-management and encouragement to continue normal activities as tolerated, so prolonged rest is usually less helpful than smart activity modification.
Myth: A quick crack or adjustment means the problem is fixed.
Fact: Temporary relief can happen, but long-term improvement usually requires restoring movement quality and load tolerance.
From the Clinic: Dr. Arora’s Expert Insight
In clinic, I often notice that patients focus on the exact fingertip point of pain and miss the movement pattern that keeps re-irritating it. Someone says, “My dimple hurts,” but when I watch them bend, stand up from a chair, carry a child on one side, get out of a car, or start walking after sitting for a long time, the real issue is usually poor load transfer between the rib cage, lumbar spine, pelvis, and hips.
What often fails is generic advice such as “just stretch,” “just strengthen your core,” or “just rest for a week.” Those instructions are too broad. What works better is first calming the irritated pattern, then restoring hip motion and trunk control, and only then reloading bending, carrying, single-leg work, and impact. When people skip that sequence, the pain near the dimples keeps returning.
What to Do About Lower Back Dimples Pain
What to do in the next 24 to 72 hours
The first goal is to reduce irritation without shutting your body down completely.
- Unload the clear aggravator. Temporarily reduce the exact movement that spikes symptoms, such as repeated twisting, deep hinging, overstriding, fast uphill walking, or asymmetrical carrying.
- Keep moving in small doses. Short, easy walks often help more than one long painful walk. A practical starting point is 5 to 10 minutes at a time, several times a day, then build as tolerated.
- Change positions before pain ramps up. If sitting is the main trigger, get up sooner. If standing is the trigger, alternate your stance and use a small foot support if helpful. If rolling in bed hurts, log-roll instead of twisting sharply.
- Use simple symptom modifiers. Some people respond better to heat for muscle guarding, while others prefer brief ice after a fresh flare. Use the one that clearly makes movement easier.
- Avoid testing the pain repeatedly. Constantly bending to “check if it is still there” often keeps the area sensitized.
Rehab plan in phases
Phase 1: Calm the flare
Use this phase when symptoms are sharp, easily triggered, or lingering after simple movements.
Exercise selection criteria:
- Choose movements that reduce pain, centralize it, or at least do not leave you worse the next day.
Good starting options:
- Diaphragmatic breathing
- Gentle pelvic tilts
- Supported hip shifts
- Small-range trunk rotation if tolerated
- Pain-free bridge isometrics
Form cues:
- Exhale first.
- Move slowly.
- Keep the range small enough that the body does not brace hard.
Regressions:
- Reduce range.
- Use pillows for support.
- Perform the movement in a more unloaded position such as hook-lying.
Phase 2: Restore motion and control
Progress here when the baseline pain is lower and flares settle within hours rather than lasting into the next day.
Targets:
- Better hip motion
- Better trunk control
- More symmetrical load acceptance through both legs
Useful options:
- Bridge progressions
- Split-stance weight shifts
- Hip-hinge patterning with a dowel
- Supported dead bug patterns
- Gentle side-lying hip work if it does not provoke the area
Form cues:
- Keep the ribs stacked over the pelvis.
- Hinge from the hips.
- Avoid pushing through the toes only.
Phase 3: Reload capacity
This is where recovery becomes more durable, but it is also where people often overdo it.
Targets:
- Bending tolerance
- Carry tolerance
- Single-leg control
- Walking pace
- Return to training or work tasks
Useful options:
- Sit-to-stand with load
- Light Romanian deadlift patterning
- Step-ups
- Suitcase carries
- Supported split squats
- Anti-rotation work
Progression rule:
- Change only one variable at a time: load, range, speed, duration, or complexity.
A good practical rule is that exercise-related soreness should stay mild and return to baseline within about 24 hours.
Phase 4: Prevent recurrence
This phase should look like your real life, not just clinic exercises.
If childcare lifting is the issue, practice floor-to-waist lifting. If desk work is the issue, build in movement breaks and trunk endurance. If running is the issue, rebuild cadence, stride length, hill exposure, and single-leg control gradually. If gym lifting triggered the flare, restore hinge mechanics before returning to heavy pulls.
Exercise selection: what makes a movement a good choice?
A good exercise for this problem does at least one of three things: it reduces pain during the session, improves movement quality, or builds the exact strength and tolerance needed for daily life. A poor exercise is one that looks impressive but repeatedly spikes symptoms, increases guarding, or does not match the actual aggravator.
That is why one person gets better with hip control and hinge work, while another improves more with flexion tolerance, walking modification, and gradual reloading of the lumbar region. The body does not care whether an exercise is trendy. It cares whether the exercise matches the problem.
Do’s and Don’ts
Do
- Keep walking in tolerable doses.
- Shorten your stride if push-off or single-leg loading hurts.
- Hinge from the hips instead of collapsing through the low back.
- Rebuild load gradually.
- Pay attention to the activity pattern that triggers symptoms.
- Get assessed if pain keeps recurring in the same region.
Don’t
- Stretch aggressively into a sharp flare.
- Assume every one-sided pain is an SI diagnosis.
- Return straight to heavy lifting, sprinting, or repeated twisting.
- Stay in bed for days.
- Rely only on short-term relief like massage, heat, or adjustments while ignoring the exercises and movement changes that address the real problem.
- Ignore bladder changes, saddle numbness, fever, or progressive weakness.
Return-to-activity guidance
Return to normal life in layers. First restore comfortable walking, transfers, and sleep. Then rebuild tolerance for bending, stairs, prolonged sitting or standing, and carrying. Only after that should you push harder into the gym, running, sports, or heavy physical work. If symptoms increase during the comeback, the answer is usually to adjust dose and mechanics, not to stop moving altogether.
When conservative care fails, and when surgery is considered
Get formal assessment if symptoms are not clearly improving after a few weeks of sensible self-management, if the pain keeps returning, if leg symptoms are increasing, or if you cannot tolerate normal work or sleep.
Surgery is rarely about the dimples themselves. NICE guideline NG59 advises against spinal fusion for routine low back pain outside a randomized trial, and recommends considering spinal decompression for sciatica only when non-surgical treatment has not improved pain or function and imaging findings fit the symptoms. For most people with mechanical regional pain around the dimples, conservative care is the main path.
Final Thoughts on Lower Back Dimples Pain
In most cases, lower back dimples pain is a sign that a nearby joint, ligament, muscle, fascia, or lumbar structure is irritated, not that the dimples themselves are abnormal. The best results usually come from identifying the aggravating movement pattern, screening for red flags, avoiding unnecessary early imaging, and following a phased rehab plan that restores control before heavy loading. If the pain is persistent, recurrent, or paired with leg symptoms or systemic warning signs, get evaluated so the true source is not missed.
FAQs
1. Can lower back dimples themselves cause pain?
Usually not. Pain in that area more often comes from nearby joints, ligaments, muscles, or referred lumbar pain.
2. Is pain near lower back dimples the same as SI joint pain?
Not always. The SI region is one common source, but facet, muscular, and referred lumbar pain can feel similar.
3. Why does the pain feel worse on one side?
One-sided pain is common and often reflects asymmetrical loading during walking, standing, lifting, or sleeping.
4. Should I get an MRI if my lower back dimples hurt?
Usually not right away. Imaging is more useful when red flags are present, symptoms persist, or the result would change treatment.
5. What movements usually aggravate this area?
Twisting while bent, prolonged standing, rolling in bed, getting out of a car, overstriding, and asymmetrical carrying are common triggers.
6. Is walking good or bad for pain around the dimples of Venus?
Walking is usually helpful in short, tolerable doses. Hills, long fast walks, or overstriding may aggravate symptoms in some people.
7. Can pregnancy or postpartum changes make this area hurt?
Yes. Pregnancy and postpartum load changes can make the SI region and pelvic ligaments more sensitive.
8. Is this pain ever related to kidney problems?
Sometimes, but not commonly. Kidney-related pain is often deeper, less movement-dependent, and may come with fever or urinary symptoms.
9. What is the fastest safe way to calm a flare-up?
Relative rest works better than full rest for most people. Reduce the trigger, change positions early, and keep moving in short tolerable doses.
10. When should I see a Physical Therapist for this?
Get assessed if pain is not improving within one to two weeks, keeps recurring, limits sleep or walking, or starts involving leg symptoms.
Medical Disclaimer
This article is for education only and does not replace individual medical assessment, diagnosis, or treatment. If you have severe pain, red-flag symptoms, or a persistent flare that is not improving, seek care from a qualified healthcare professional.
References
- Dimple of Venus Is Associated with the Increased Pelvic Incidence Angle and More Sagittally Oriented Facet Joint (https://pubmed.ncbi.nlm.nih.gov/37285829/)
- Low back pain and sciatica in over 16s: assessment and management (NICE guideline NG59) (https://www.nice.org.uk/guidance/ng59/chapter/recommendations)