“Expert Review: This article includes clinical insights from Dr. Arora, a physiotherapist with 20+ years of experience.”
Elliptical machine lower back pain is caused by the lumbar spine taking over as a stabilizer when the hips and glutes stop doing their job. This happens due to poor posture on the machine, handles set too high or too low, excessive stride length, or glute fatigue during longer sessions. The elliptical is low-impact but still demands continuous trunk control — and when that control breaks down, the lower back pays the price
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult a healthcare professional before starting a new exercise or rehab program.
If you’re experiencing lumbar pain during your elliptical workouts, the goal isn’t to “push through” or abandon cardio. It’s to pinpoint what’s provoking your back (setup, posture, stride, intensity, or fatigue), fix the mechanics, and rebuild capacity so your hips and trunk share the work again.

What the elliptical changes in your body (and why your back notices)
1) It’s a “fixed-foot glide,” not normal walking
On an elliptical, your feet stay planted on moving pedals. That changes how force travels through your legs and how your pelvis needs to control rotation. Research comparing elliptical exercise with level walking shows different lower-limb joint loading patterns, which helps explain why one mode can feel fine while the other irritates symptoms (Lu et al., 2007).
2) Small setup choices can change spinal motion and muscle demand
Hand position, speed, and stride length influence trunk mechanics and muscle activity during elliptical use (Moreside et al., 2012). Clinically, this is why “leaning on the handles” or “reaching too far forward” can quickly turn an easy workout into a back-aggravating one.
3) “Low impact” can still mean “high endurance demand”
Even when impact is reduced, the elliptical can demand sustained trunk control—especially at high resistance, high incline, or slow grinding cadence. If your glutes fatigue and your breathing becomes shallow, the spine stiffens to compensate. If tight glutes are already a problem before you get on the machine, the elliptical will make it worse faster.
Over 10–30 minutes, that’s a common pathway to back aches during gliding.
Two common patterns of lower-back irritation on cardio machines
Not everyone’s back behaves the same. A useful clinical lens is to identify whether you’re more extension-sensitive or flexion-sensitive, because the elliptical can bias you toward either—depending on your posture and fatigue.
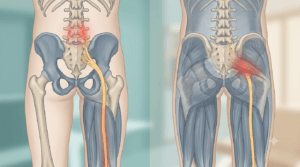
Extension-sensitive (“pinch/pressure” type)
Typical feel: localized ache or pinching near the belt line; worse with incline, leaning back, rib flare, or “standing tall with an arch.”
Common driver: excessive lumbar extension and facet compression during repetitive loading.
Flexion-sensitive (“stretch/leggy” type)
Typical feel: ache that can spread into buttock or thigh; worse with slumping, rounded posture, long sitting, or poor hip hinge.
Common driver: sustained flexion load and poor segmental tolerance (especially if you already dislike sitting).
Why this matters: prevention is faster when you match the strategy to the pattern.
Elliptical machine lower back pain: 9 common triggers and the exact fix for each
Most lower-back issues on the elliptical come from two themes:
- losing a stable ribs-over-pelvis “stack,” and
- borrowing motion from the lumbar spine when the hips should be doing it.
Use this like a checklist. Most people have 2–3 contributors.
1) Hanging on the handles (the “support rail” problem)
What it feels like: belt-line ache or pinching that builds quickly, especially on incline.
Why it happens: leaning forward or loading your bodyweight through the arms often flares the ribcage and increases lumbar extension.
Fix (next session):
- Use light fingertip contact, not a weight-bearing grip.
- Exhale gently to bring ribs down without slumping.
- Lower incline first; rebuild time before intensity.
2) Stride is too long (hips run out of extension)
What it feels like: pinchy discomfort at the back of the stroke; sometimes one-sided.
Why it happens: long stride increases hip extension demand. If the hip can’t give it, the low back substitutes with extension/rotation.
Fix:
- Stand slightly more centered and shorten the stroke.
- Keep a soft knee at end range (avoid “locking out”).
- Prefer smooth cadence over slow grinding.
3) Excess incline + resistance (turning it into a “spine grind”)
What it feels like: deep fatigue and aching that ramps up over time.
Why it happens: heavy settings increase sustained trunk stiffness demand.
Fix:
- Reduce one variable at a time: flatten incline or drop resistance.
- Keep a cadence you can breathe through (no breath-holding).
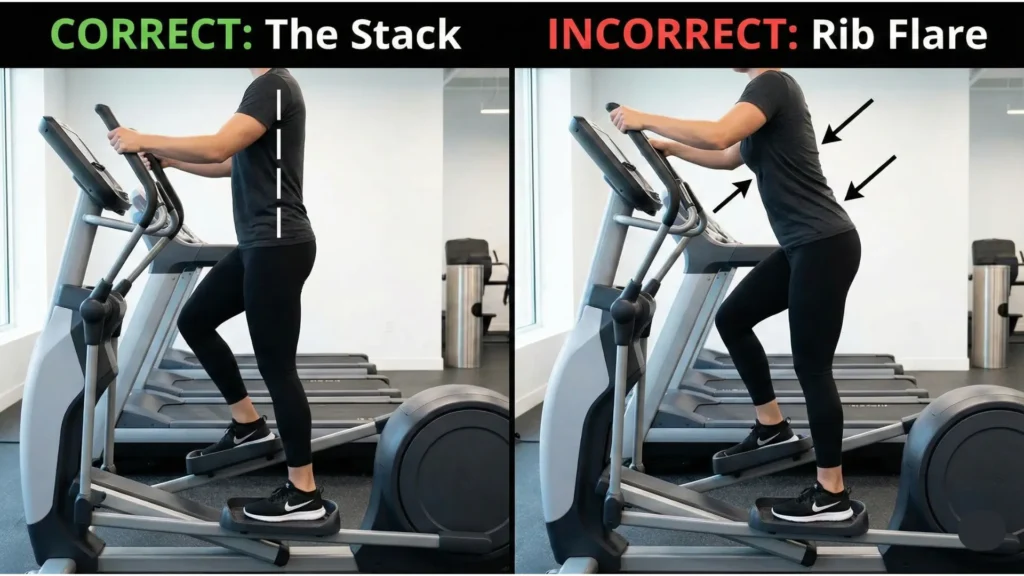
4) Rib flare and over-arching (extension bias)
What it feels like: pressure/pinch that improves when you step off and flex slightly.
Why it happens: rib flare increases lumbar lordosis and facet compression—common in people trying to “stand tall.”
Fix:
- Think “zip ribs down” (gentle, not forced).
- Keep pelvis neutral; avoid a hard tuck or hard arch.
- Use short intervals until control improves.
5) Hip flexors dominate (front-of-hip tightness + back pressure)
What it feels like: front-hip pull plus low-back ache.
Why it happens: hip flexors overwork; glutes under-contribute; pelvis drifts forward. Also, stretching hip flexors doesn’t reliably create large posture changes for everyone (Preece et al., 2021).
Fix:
- Cue “push the pedal back with the glute,” not “pull up with the front hip.”
- Add glute-biased intervals (below).
- Stretch gently after training only if it helps.
6) Glute fatigue → pelvic wobble (loss of lumbopelvic control)
What it feels like: fine for 5–10 minutes, then symptoms appear as form falls apart.
Why it happens: pelvic drop/rotation increases when glutes fatigue; the spine stiffens to compensate.
Fix:
- Switch to intervals: 2 min easy / 1 min moderate.
- Keep pelvis “quiet” (no visible sway).
- Add side-hip endurance off the machine.
7) Over-bracing + shallow breathing (stiff trunk, quick fatigue)
What it feels like: tight back, shallow breathing, sometimes spasm.
Why it happens: max-effort bracing for long durations increases compression and fatigue.
Fix:
- Brace at 30–40% (“support,” not “armor”).
- Breathe low and wide (360° expansion).
8) Asymmetrical foot pressure (pelvis twists every cycle)
What it feels like: one-sided ache, sometimes near the SI region.
Why it happens: uneven pressure drives repeated pelvic rotation thousands of times.
Fix:
- Match foot angle on both pedals.
- Use a “tripod foot” cue: heel + big toe + little toe.
- Keep knees tracking over the second toe.
9) Too much, too soon (the delayed flare pattern)
What it feels like: okay during the workout, worse later that day or next morning.
Why it happens: the session exceeded recovery capacity.
Fix:
- Build minutes before intensity.
- Increase only one variable every 3 sessions.
- Use the 24-hour rule: if next-day symptoms spike, step back.
A 2-minute self-check before your next session
Step 1: When does discomfort start?
- 0–2 minutes: setup/posture driver
- 8–15 minutes: endurance/capacity driver
- Later that day / next morning: progression/recovery driver
Step 2: Where do you feel it?
- Center belt line: often compression/stiffness pattern
- One-sided “dimple” area: often facet/SI irritation
- Below the knee: possible nerve sensitivity → be conservative
Step 3: What changes it immediately?
Try one change for 60 seconds:
- lighter hand contact / stop leaning
- reduce incline by 2–3 levels
- raise cadence slightly and reduce resistance
If symptoms drop meaningfully, you’ve found a mechanical driver you can control.
Red flags: when to stop and get assessed
Stop exercising and seek urgent evaluation if you have:
- new bowel/bladder changes, saddle numbness, or rapidly worsening leg weakness
- fever, unexplained weight loss, history of cancer, or significant trauma
- severe night pain that doesn’t change with position
- rapidly progressive numbness/tingling or weakness
Also seek assessment if symptoms are escalating week-to-week or consistently radiate into the leg.
From the Clinic: Dr. Arora’s Expert Insight
The biggest pattern I see isn’t “weak core”—it’s fear-driven strategy. People brace too hard, stop breathing, and then lean onto the handles to feel stable. That shifts the ribcage forward and the pelvis into an exaggerated arch, turning the lumbar spine into a load-bearing column for the entire session.
The cue that works best is: stack, breathe, then drive with the hips. When someone can keep ribs over pelvis and breathe under effort, glutes contribute again and symptoms settle. If you can hold good form for only 6–8 minutes right now, that’s simply your current capacity. We build from that instead of forcing 25 minutes and flaring.
Prevention plan: a setup + technique system you can repeat
Step 1 — Set the machine for control (not ego)
- Incline: start flatter (0–4) until symptom-stable
- Resistance: low enough to breathe normally
- Cadence: smooth and moderate (avoid grinding)
- Hands: light contact to start; add moving handles later
Step 2 — Use the “stack” cue
- Exhale gently and let the lower ribs soften down
- Keep pelvis neutral (no hard tuck, no hard arch)
- Stay tall through the crown of the head
Step 3 — Make the hips do the work
- “Push the pedal back with the butt” (glute)
- Quiet pelvis (no side-to-side sway)
- Even foot pressure (tripod foot)
A simple 2-week return-to-elliptical plan
Week 1 — Restore tolerance
- Total: 12–18 minutes
- Intervals: 2 min easy / 1 min moderate × 6
- Settings: low resistance, low incline
- Rule: finish with the same symptoms you started with (not worse)
Week 2 — Build capacity
- Total: 18–25 minutes
- Intervals: 3 min easy / 1 min moderate × 6
- Progression: change only one variable every 3 sessions
- 24-hour check: if next-day symptoms jump, step back one level
Off-machine rehab: 6 exercises that make the elliptical feel “easy”
Pick one from each category and do them 3–4 days/week. If your main issue is related to poor elliptical form, these drills give the fastest return on effort.
A) Trunk control (reduce extension and rotation “leaks”)
1) Dead bug with breathing (anti-extension)
- 6–8 reps/side, slow
- Exhale as the leg reaches; keep ribs down without forced flattening

2) Side plank (anti-rotation)
- 20–30 seconds × 3
- Feel side hip + oblique, not low-back pinch
Core stability exercise has shown short-term benefits over general exercise for pain/function in chronic low back pain in meta-analytic work (Wang et al., 2012).
B) Hip mobility + hinge pattern (give motion back to hips)
3) Half-kneeling hip flexor stretch (gentle)
- 30–45 seconds × 2/side
- Squeeze back-leg glute; avoid arching the low back
4) Hip hinge drill (teach “hips, not spine”)
- 8–10 reps × 2
- Ribs stacked; send hips back; stop before rounding/arching
C) Glute endurance (pelvic stability)
5) Glute bridge with 3-second holds
- 10 reps × 2
- Stop if hamstrings cramp; feel butt, not toes
6) Band lateral walks
- 8–12 steps each way × 2
- Level pelvis; small steps; knees track over toes
Do’s and Don’ts for staying symptom-stable on the elliptical
| Do | Don’t |
|---|---|
| Start flatter and lighter than you think | Use the handles as a support rail |
| Use intervals when rebuilding tolerance | Combine high incline + high resistance while symptomatic |
| Keep a tall “stack” and breathe during effort | Grind slow, heavy strokes with breath-holding |
| Stop sets when your pelvis starts to sway | Force a long stride if hips feel tight |
| Progress one variable at a time | Ignore progressive leg symptoms (numbness/weakness) |
Myths vs facts
Myth: “If the elliptical bothers my back, it’s a bad machine.”
Fact: It’s usually a mismatch between setup/technique and current capacity. When mechanics improve and endurance builds, many people return comfortably.
Myth: “I just need to stretch hip flexors.”
Fact: Mobility can help, but endurance, breathing, and pelvic control are often bigger levers. Hip flexor stretching alone doesn’t reliably change pelvic tilt/lordosis for everyone (Preece et al., 2021).
Myth: “Bracing harder always protects the spine.”
Fact: Over-bracing for long durations increases fatigue and can increase compression. Controlled bracing + breathing is usually safer.
Elliptical vs treadmill vs bike for back pain: which is safer?
There’s no universal winner; the best option is the one you can do with stable mechanics and predictable recovery.
- Elliptical: lower impact; technique-sensitive; can bias extension if you lean
- Treadmill walking: highly adjustable; often easiest to keep a natural hip strategy
- Upright bike: may suit extension-sensitive backs; can irritate flexion-sensitive backs if you slump
Studies comparing walking and elliptical training show meaningful differences in joint kinematics and muscle demands (Burnfield et al., 2010), which supports why one mode may feel better than another for the same person.
Conclusion
If your workouts keep triggering elliptical machine lower back pain, the fix is rarely “stop cardio forever.” It’s almost always a combination of (1) correcting the mechanical driver (leaning, rib flare, stride length, intensity), (2) rebuilding capacity with smart intervals, and (3) improving trunk + glute endurance so your spine doesn’t carry the session. Apply the stack-and-breathe cues, start flatter and lighter, progress one variable at a time, and your back response should become predictable—and preventable.
FAQ
1) Why does the elliptical irritate my back but walking doesn’t?
Because your feet are fixed to the pedals, which changes hip motion and trunk demand. That difference is often enough to provoke symptoms if your mechanics drift.
2) Should I stop immediately if I feel a pinch?
If the pinch is increasing, stop and reset. First try flattening incline, lowering resistance, and removing handle “support.” If it doesn’t settle, end the session.
3) Are moving handles better or worse?
They can help if they keep you upright and breathing. They can worsen symptoms if they make you lean, reach, or hang for support.
4) What’s the safest starting setup after a flare?
Low incline, low resistance, smooth cadence, and intervals. Your goal is symptom-stable tolerance, not intensity.
5) Is it normal to feel sore the next day?
Mild muscle soreness can be normal. A clear pain flare usually means you progressed too fast. Reduce one variable and rebuild.
6) Should I stretch before or after?
If you’re irritable, aggressive stretching before can make you feel looser but less stable. Many people do better with gentle mobility after.
7) Can shoes affect back symptoms on the elliptical?
Yes. Unstable shoes can change foot pressure and knee tracking, which can translate into pelvic rotation over time.
8) Is backward pedaling worth trying?
It can change muscle emphasis. Try it briefly at low resistance while maintaining posture; stop if symptoms rise.
9) What are the best strength exercises to support cardio?
Consistent trunk control (anti-extension/anti-rotation) and glute endurance. Keep it simple and repeatable.
10) When should I seek help?
If symptoms radiate below the knee, you notice numbness/weakness, red flags appear, or the problem persists beyond 2–3 weeks despite correct progression.
References (Primary scientific literature)
- Lu TW, et al. Joint loading in the lower extremities during elliptical exercise (2007).
- Moreside JM, et al. How do elliptical machines differ from walking: a study of hand position, stride length and speed (2012).
- Burnfield JM, et al. Similarity of joint kinematics and muscle demands between walking and elliptical training (2010).
- Preece SJ, et al. Comparison of pelvic tilt before and after hip flexor stretching (2021).
- Wang XQ, et al. A meta-analysis of core stability exercise versus general exercise for chronic low back pain (2012).