“Expert Review: This article includes clinical insights from Dr. Arora, a physiotherapist with 20+ years of experience.”
If your back suddenly feels tight, achy, or “stuck” on a hot day—or after a long flight, a stomach bug, or a sweaty workout—you’re not imagining it. The connection between dehydration and lower back pain is real, but it’s often misunderstood. Many people label the sensation as lower back pain from dehydration or search phrases like not drinking enough water back pain when the flare seems to track with busy, low-fluid days.
Here’s the key: dehydration rarely “injures” your spine in isolation. Instead, low fluid intake (and sometimes low electrolytes) makes muscles more irritable, reduces your tolerance to sitting, and amplifies the nervous system’s protective guarding.
If your symptoms line up with the patterns below, it’s reasonable to treat dehydration in order to relieve lower back pain.
In my clinic, people commonly arrive convinced they’ve “slipped a disc.” Then we map the last 24–72 hours: heat exposure, less water, more caffeine/alcohol, poor sleep, long sitting, and maybe one awkward lift. That stack is how a back flare starts—without any major tissue damage.
This guide will help you:
- Understand how hydration status can influence symptoms
- Spot the 9 signs your pain is at least partly a fluid problem
- Separate muscle/joint pain from kidney/urinary red flags
- Use a practical 24-hour reset and a 2-week prevention plan

Dehydration and lower back pain: what’s really going on?
When patients ask, “Can dehydration cause lower back pain?” the most accurate answer is: yes, it can contribute, usually through indirect pathways. The phrase dehydration and lower back pain is best understood as a state problem—your body’s recovery and chemistry—rather than a single damaged structure.
The three pathways that create the “fluid → back pain” pattern
1) Muscle irritability and protective spasm
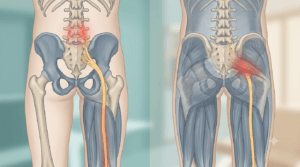
Muscle contraction depends on water, sodium, potassium, calcium, and magnesium moving across cell membranes. When you’re under-hydrated (or you’ve sweated out sodium and replace only with water), muscles can fatigue sooner and become more excitable. The lumbar extensors and hip flexors are especially vulnerable because they work all day at low intensity to keep you upright.
This is why dehydration and lower back pain often show up as:
- crampy, tight, “rope-like” discomfort
- worse with prolonged standing or end-of-day fatigue
- better with gentle walking and recovery inputs
In controlled research after heat/exercise dehydration, water-only rehydration increased muscle cramp susceptibility, while an electrolyte-containing solution reversed that effect.¹ This is a big reason dehydration and lower back pain can feel like your back is “gripping” rather than “injured.”
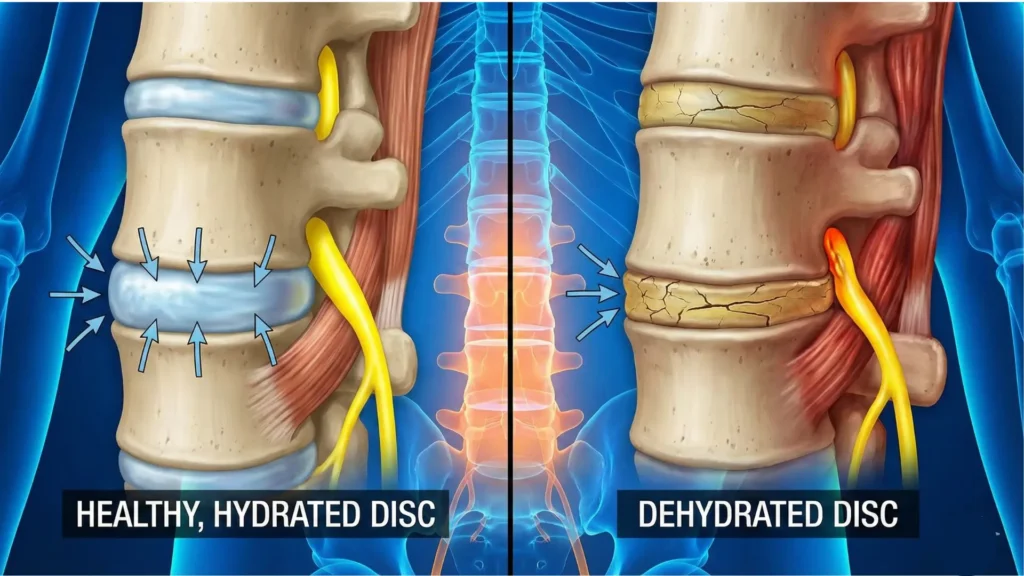
2) Disc and tissue load tolerance shifts
Your intervertebral discs behave like fluid cushions. They naturally lose water under compression during the day and recover during rest. Quantitative MRI work shows measurable diurnal variation in lumbar disc water-related signals.²
This doesn’t mean one glass of water instantly “rehydrates” a disc. It means your spine’s tissues have normal fluid dynamics—and when your overall recovery state is poor, the same posture and load can feel far more irritating. That’s why dehydration and lower back pain often show up after long sitting, bending-heavy chores, or travel days.
3) Kidney and urinary conditions mimicking back pain
Dehydration can concentrate urine and increase the risk of kidney stones in susceptible people. It can also worsen kidney stress when paired with heat illness. Mechanistic research describes pathways by which recurrent dehydration may contribute to kidney injury over time.⁴
This matters because not every “back ache on a dehydrated day” is musculoskeletal. In some cases, dehydration and lower back pain is the wrong frame entirely—what you actually need is a urine test and medical evaluation.
Why your back feels worse on travel days, hot days, or “busy weeks”
A recurring theme in dehydration and lower back pain is that it appears during life bottlenecks. When you see repeat flares on “hot, travel, or busy” days, dehydration and lower back pain becomes a very practical working label.
- Heat + sweat: fluid loss + electrolyte loss + fatigue
- Flights/long drives: low fluid intake + prolonged sitting + stiff hips
- Alcohol/caffeine: diuretic effect + sleep disruption + increased muscle tone
- Illness (vomiting/diarrhea): rapid fluid/electrolyte shifts
- Long desk days: dehydration + static posture + reduced movement breaks
The hidden mechanical amplifier: stooped posture
When you sit slumped for hours, you load spinal tissues in flexion. Research on simulated stooped posture has shown changes consistent with reduced disc hydration under that posture compared to erect posture.³ That doesn’t mean “sitting causes disc damage,” but it helps explain why dehydration and lower back pain commonly appear together on days you’re both under-hydrated and stuck in flexion.
The kidney vs muscle decision: don’t miss this
People often search dehydration kidney pain vs back pain because the location is confusing. Here’s a practical screen.
More consistent with muscle/joint-driven back pain
- Pain across the beltline or buttock area
- Stiffness after sitting; eases with gentle walking
- Tender muscles when you press
- Pain changes clearly with movement/position
More consistent with kidney/urinary causes
- Higher pain under the ribs toward one side (flank)
- Pain doesn’t reliably change with posture
- Fever/chills, nausea/vomiting
- Burning/urgency/frequency, or blood in urine
If you have urinary symptoms, fever, severe one-sided flank pain, or vomiting that prevents hydration, don’t treat it as “just dehydration and lower back pain.” Get medical care.
9 signs your back pain is a fluid problem
These signs don’t prove dehydration is the only cause. They help you identify when hydration, electrolytes, and recovery are meaningful levers—so you don’t waste weeks chasing the wrong solution. Think of them as the most common dehydration and lower back pain clues.
1) Your flare happens on hot days or after heavy sweating
If symptoms reliably appear after heat exposure, outdoor work, long walks in summer, sauna, or intense workouts, the dehydration and lower back pain pattern is likely. Sweat loss reduces plasma volume, increases fatigue, and can raise protective muscle tone.
2) Thirst and darker urine show up the same day
Urine color isn’t a perfect hydration marker (some vitamins darken urine), but timing matters. If thirst + darker urine + low intake coincide with onset, treat hydration as a real contributor to your flare. Sustained low fluid intake can itself contribute to back pain — our article on dehydration and lower back pain explains what fluid loss does to spinal discs.
3) The pain feels tight, band-like, or crampy rather than sharp
Fluid-related flares often feel like:
- tight bands across the beltline
- “pressure” or “gripping”
- stiffness during transitions (sit-to-stand)
Sharp, pinpoint pain can still happen, but crampy tightness is classic for dehydration and lower back pain episodes.
4) You’re cramping or twitching in other muscles too
If calves, hamstrings, or feet are cramping, the lumbar muscles may be in the same irritability state. People commonly describe this as dehydration muscle cramps lower back—a gripping beltline tightness that improves once fluids and electrolytes normalize.
Controlled dehydration research shows rehydration strategy can influence cramp susceptibility.¹ This is where dehydration and lower back pain overlaps with electrolyte balance: nerves and muscles need both fluid and minerals.
5) Travel days trigger stiffness and flare-ups
Flights and long drives combine dry air, less drinking, static posture, and awkward lifting. This stack is one of the most common setups for lower back pain due to dehydration.
6) You improve noticeably within 12–24 hours of smart rehydration
Time course is a strong clue. If symptoms drop significantly by the next day after steady fluids, electrolyte support when appropriate, and gentle movement, dehydration and under-recovery were likely major drivers of the episode.
7) You also feel headachy, lightheaded, or unusually fatigued
Back pain can exhaust you, but dehydration often adds systemic signals: headache, dizziness on standing, “heavy legs,” or brain fog. If these co-occur with back tightness, lower back pain is due to dehydration is a reasonable working hypothesis.
8) The episode started after vomiting, diarrhea, fasting, or a crash diet
GI illness and restrictive dieting can shift fluid and electrolytes quickly. If the timeline fits, don’t assume your spine is “fragile.” Often this is driven by a short-term chemistry and recovery deficit.
9) You notice urinary changes with the back pain
Burning, urgency, fever, nausea, or blood in urine shifts the probability toward urinary/kidney causes. Don’t self-manage this as dehydration and lower back pain—get assessed.
Myths vs facts
Myth: “If I drink water, my discs rehydrate immediately.”
Fact: Disc hydration is influenced by unloading/rest and disc biology. Diurnal changes in lumbar disc water content are measurable on MRI.² Hydration is part of the system, but it isn’t an instant fix.
Myth: “Dehydration is the main cause of back pain.”
Fact: Most low back pain is multifactorial: load, sleep, stress, conditioning, and tissue sensitivity. Dehydration and lower back pain often co-exist because dehydration amplifies those factors—not because dehydration is always the root cause.
Myth: “More water is always better.”
Fact: If you’ve lost electrolytes through heavy sweating or illness, replacing only water can worsen symptoms in some people. A controlled study found electrolyte-containing rehydration reversed increased cramp susceptibility seen with water-only intake.¹
From the Clinic: Dr. Arora’s Expert Insight
At Korba Spine & Joint Centre, the patients who match the dehydration and lower back pain pattern rarely say “I’m thirsty.” They say, “My back suddenly locked up.” When I ask about the last 48 hours, it’s usually heat exposure or travel, long sitting, irregular meals, low fluids, and poor sleep—then one routine bend becomes the tipping point.
The common mistake is treating hydration like an emergency button: drinking very little all day, then chugging plain water at night once pain hits. That approach often fails because the nervous system is already guarding—and because sweat/illness losses often require electrolytes too. When we correct the basics (steady intake, sensible electrolyte support, and a short movement plan), these flares become predictable and preventable.
What to do today: a safe 24-hour reset
If you have fever, urinary symptoms, severe one-sided flank pain, fainting, confusion, or neurological red flags (new weakness, saddle numbness, bowel/bladder changes), skip self-care and seek urgent evaluation.
Step 1: Rehydrate steadily (don’t chug)
A practical approach for most adults
- Sip water through the day rather than forcing large amounts at once.
- If you’ve had heavy sweating, diarrhea, or recurring cramps, use an oral rehydration solution or electrolyte drink. This is where electrolyte imbalance and back pain becomes clinically relevant—water alone isn’t always the right replacement after heavy sweat or GI losses.
This matters because dehydration often include muscle excitability, and rehydration strategy can influence cramp susceptibility.¹ When you manage dehydration early, you often shorten the whole flare.
Do not “overcorrect”
If you have heart failure, kidney disease, or fluid restrictions, follow clinician guidance.
Step 2: De-threaten the spine with low-load movement (10 minutes)
The goal is to reduce guarding without provoking pain.
2A) Crook-lying breathing (2–3 minutes)
- Lie on your back, knees bent.
- Inhale gently; exhale longer.
- Let ribs soften down on the exhale (don’t brace hard).
2B) Pelvic tilts (1–2 sets of 8–10)
- Rock pelvis to flatten the low back slightly, then return to neutral.
- Keep it small and smooth.
2C) Easy walking (5 minutes)
- Relaxed pace; even breathing.
This combination is often enough to take the edge off dehydration and lower back pain guarding within hours.
Step 3: Reduce compression triggers for 24 hours
For one day, avoid:
- prolonged sitting without breaks
- deep end-range stretching if you’re cramping
- heavy lifting from a rounded back
Instead:
- stand and walk 60–90 seconds every 30–45 minutes
- practice a gentle hip hinge when you bend
Step 4: Sleep position that unloads the back
- Side-lying with pillow between knees, or
- On your back with pillow under knees
Since discs show measurable diurnal water variation,² unloading plus sleep quality matters when you’re managing dehydration and lower back pain.
A 2-week prevention plan (so it doesn’t keep coming back)
Week 1: Make hydration automatic + restore tolerance
Hydration habit (simple and repeatable)
- 1 glass on waking
- 1 mid-morning
- 1 mid-afternoon
- 1 with dinner
On heat/sweat days, increase intake and consider electrolytes. If your pattern is dehydration that leads to lower back pain, consistency beats “rescue chugging.” In other words, dehydration and lower back pain improves most when hydration becomes boring and routine.
Movement habit (10 minutes/day)
- 5 minutes walking
- 2 minutes breathing reset
- 3 minutes pelvic tilts + hip hinge rehearsal
Week 2: Build capacity (3 days/week)
Choose loads that feel “easy enough to repeat.”
Strength circuit
- Glute bridge: 2–3 × 8–12
- Supported split squat (hands on wall): 2 × 6–8 each side
- Light farmer carry: 4 × 30–60 seconds
Capacity work matters because dehydration and lower back pain is often the spark, but low tissue tolerance is the fuel.
Do’s and don’ts
Do
- Do spread fluid intake across the day.
- Do add electrolytes when sweating is heavy or cramps are recurring.
- Do use low-load movement early (walking, pelvic tilts).
- Do protect sleep on recovery days.
- Do treat travel and heat days as “higher risk” if you’ve had dehydration and lower back pain before.
Don’t
- Don’t ignore fever, urinary symptoms, or blood in urine.
- Don’t do heavy deadlifts “to loosen it” in the first 48 hours.
- Don’t aggressively stretch a cramping lumbar region.
- Don’t mask symptoms with painkillers while ignoring dehydration or illness.
Conclusion
Most episodes that look like a “mystery back injury” are actually a predictable stack: low fluids, poor sleep, long sitting, and a sudden load. That’s why dehydration and lower back pain is a useful frame—because it reminds you to fix recovery inputs and mechanics.
If your flare pattern matches the signs above, start with steady rehydration, electrolyte support when appropriate, gentle movement, and 24 hours of reduced compression. Then rebuild capacity for two weeks. Do that consistently, and most people find their dehydration and lower back pain episodes become less frequent, less intense, and far less scary.
FAQ
1) Can dehydration cause lower back pain even if I didn’t exercise?
Yes. Heat exposure, travel, alcohol, low intake, or illness can create a recovery deficit that increases guarding and tissue sensitivity. That’s one common pathway for dehydration and lower back pain.
2) How do I know it’s dehydration and not a disc problem?
If symptoms improve within 12–24 hours after steady fluids, gentle walking, and better sleep, it’s usually a state-dependent flare rather than structural damage. Disc hydration also follows normal diurnal changes.²
3) Is kidney pain the same as back pain from dehydration?
Not always. Kidney/urinary pain is often higher and more one-sided (flank) and may come with fever, nausea, or urinary symptoms. If those are present, get evaluated rather than self-treating.
4) Should I drink only water or add electrolytes?
If you’ve been sweating heavily, had diarrhea/vomiting, or are cramp-prone, electrolytes can matter. A controlled dehydration study showed an electrolyte drink reversed increased cramp susceptibility seen with water-only intake.¹
5) How quickly should I feel better?
Many people feel noticeable improvement within 12–24 hours if dehydration and muscle guarding were major contributors. If pain worsens, persists beyond a few days, or red flags appear, seek evaluation.
6) Can sitting make this worse even if I’m hydrated?
Yes. Stooped sitting can increase flexion load and has been linked to hydration-related changes in discs under simulated conditions.³ Long sitting plus low movement breaks can trigger dehydration and lower back pain episodes even with decent water intake.
7) Why is my back stiffer at the end of the day?
Discs lose water under compression during the day and recover with rest; diurnal disc water changes are measurable.² Add fatigue and low fluids, and the system feels less tolerant—classic dehydration and lower back pain timing.
8) Can I keep working out during a flare?
Often yes—but scale it. Avoid heavy spinal loading for 24–48 hours, prioritize walking and low-load movement, and reintroduce strength when pain is settling. If symptoms include neurological deficits, stop and get assessed.
9) What are the red flags that mean I should not self-treat?
Fever/chills, vomiting preventing hydration, blood in urine, severe one-sided flank pain, new weakness, saddle numbness, or bowel/bladder changes.
10) What’s the best long-term prevention strategy?
Make hydration consistent, use electrolytes when sweating is heavy, break up sitting, and build hip/glute/trunk capacity. Long-term, the best protection against dehydration and lower back pain is a body that tolerates load even on “imperfect” days—and a routine that prevents dehydration from becoming the repeat trigger for back pain.
References:
- Water intake after dehydration makes muscles more susceptible to cramp but electrolytes reverse that effect (2019)
- Segmental Quantitative MR Imaging Analysis of Diurnal Variation of Water Content in the Lumbar Intervertebral Discs (2015)
- Spinal disc hydration status during simulated stooped posture (2012)
- Mechanisms by Which Dehydration May Lead to Chronic Kidney Disease (2015)
- Effect of Hydration on Healthy Intervertebral Disk Mechanical Stiffness (2015)