If you typed body leaning to one side lower back pain, you’re describing a very specific flare-up pattern: your trunk drifts left or right, and standing “straight” feels blocked or sharply painful. People also phrase it as “leaning to one side with lower back pain” or “walking bent to one side back pain,” but the core concern is the same—why am I crooked, and how do I safely get back to center?
Most of the time, body leaning to one side lower back pain is not a permanent deformity. It’s a protective posture your nervous system adopts to unload an irritated structure (often disc/nerve tissue). The key is doing the right thing in the right order, because the wrong order can worsen symptoms.
This guide explains:
and the correct treatment sequence: Plan A (shift correction) → Plan B (extension to lock it in).
what a true lateral shift is (and what it isn’t),
safe home checks (without risky balance tests),
“Expert Review: This article includes clinical insights from Dr. Arora, a physiotherapist with 20+ years of experience.”

What “body leaning to one side lower back pain” usually means
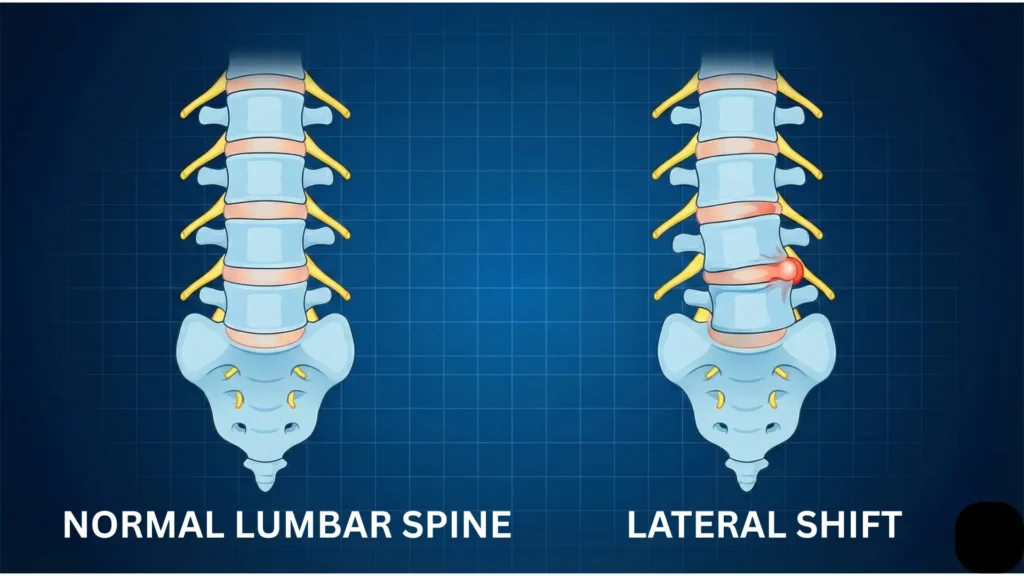
Clinically, a fixed crooked posture—where your shoulders are laterally offset from your pelvis even when standing still—is often called a lateral shift or trunk list. This pattern is widely discussed as being associated with disc-related pain presentations, including cases where symptoms change meaningfully once the shift is corrected.
The pattern in simple anatomical terms
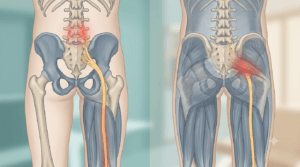
Your lumbar spine has vertebrae (bones) with discs in between. Nerve roots exit the spine close to the discs and travel toward the buttock and leg. When disc/nerve tissues become highly irritable, the body often adopts a posture that reduces irritation—sometimes by shifting the trunk sideways.
That’s why body leaning to one side lower back pain can feel involuntary: you’re not choosing to be crooked; you’re defaulting into a position your nervous system currently perceives as safest.
Typical signs of a true lateral shift
- You look crooked in the mirror with shoulders shifted left/right relative to hips
- The “crookedness” remains even when you’re not walking
- Attempting to straighten feels blocked, sharp, or triggers leg symptoms
- Walking feels awkward and guarded (walking bent to one side back pain)
- One side-glide direction feels “jammed,” not just tight
Why trunk list matters (and what it suggests)
In a classic clinical study of patients with back pain and trunk list, a substantial portion met criteria consistent with a symptomatic lumbar disc lesion, and the direction of the list did not reliably match the side of sciatica.
So the posture is meaningful, but it’s not a perfect “map” of side/level by itself.
SI joint vs. lateral shift: the difference that prevents wrong self-diagnosis
This is where many articles confuse readers, so let’s separate them clearly.
A true lateral shift (fixed crooked posture)
- Shoulders are offset from pelvis even when standing still
- The posture feels “locked”
- Often behaves like a disc/nerve sensitivity problem (symptoms may centralize/peripheralize with repeated movements)
- Correction typically requires pelvis repositioning under ribcage before extension work
An antalgic lean (pain-avoidance limp)
SI joint pain and hip pain more commonly create a weight-bearing avoidance pattern, not a fixed trunk list:
- You lean away from the painful side when you step on it
- You may limp
- You may show a Trendelenburg pattern (pelvis drops on one side due to hip abductor pain/weakness)
- When standing still with equal weight, you may look more centered than you do while walking
Bottom line: SI/hip problems can absolutely change your gait and make you “lean,” but a fixed crooked posture while standing still is more consistent with a lateral shift pattern than with isolated SI dysfunction.
Common causes of body leaning to one side lower back pain
1) Disc/nerve irritation with a lateral shift pattern (most classic)
A sudden bend/lift/twist may trigger pain, then you notice body leaning to one side lower back pain and can’t straighten. Case-based clinical literature describes that correction of the lateral shift is often the first target before progressing to extension-based loading.
Clues
- Pain may spread to buttock/thigh/calf (not always)
- Cough/sneeze/strain can spike pain
- One direction of movement clearly worsens leg symptoms (peripheralization)
2) One-sided muscle guarding and spasm (can mimic the look)
Protective spasm can pull you into body leaning to one side lower back pain, but usually it feels more like a tight clamp and less like a “mechanical block” with leg symptoms.
Clues
- More local pain near the spine or iliac crest
- Heat + gentle walking helps
- No consistent below-knee symptoms
3) Facet irritation (extension/rotation sensitive)
Can create sharp one-sided back pain and guarded posture.
Clues
- Worse with arching/twisting
- Better with slight flexion for many
4) Hip drivers (glute med pain/weakness, hip impingement)
More likely to cause an antalgic lean during walking than a fixed trunk list.
Clues
- Lateral hip/groin pain
- Limp increases with fatigue
- Single-leg stance is painful/unstable
5) Less common but important causes
Fracture, infection, inflammatory disease, or tumor are uncommon but serious. If symptoms don’t change with position, or you have systemic red flags, don’t self-treat.
Red flags: when body leaning to one side lower back pain needs urgent care
Get urgent evaluation if you have:
- new bowel/bladder changes
- saddle numbness (groin/inner thighs)
- progressive leg weakness
- fever/chills or systemic illness signs
- major trauma
- history of cancer or immune suppression
- severe constant pain unaffected by position
Safer home checks (no risky balance tests)
These are not diagnostic. They help you decide whether you’re likely dealing with a true shift and how your symptoms respond.
1) Mirror “fixed shift” check
Stand still (not walking). Look for:
- shoulders shifted left/right relative to hips
- inability to return to center without sharp block
2) Side-glide stiffness check (tiny range only)
Without twisting, try a small pelvis glide left and right.
If one direction is sharply blocked or increases leg symptoms, treat that as useful information.
3) Walking tolerance check (2 minutes)
Walk gently:
- Do you loosen slightly after 60–90 seconds?
- Or do symptoms spread further down the leg?
4) Static strength check (supported)
Instead of heel-walking/toe-walking:
- Hold a kitchen counter
- Lift your toes up (ankle dorsiflexion) one foot at a time
- Lift your heels up (calf raise) one foot at a time
If you cannot lift on one side or it feels suddenly weak compared to the other, get assessed.
5) Centralization check (high value)
Centralization = symptoms retreat from leg/buttock toward the back with repeated movement. This phenomenon has been shown to have prognostic and clinical value in low back pain populations.
Try 8–10 gentle reps of the “least-bad” movement (only if safe). If leg pain moves upward or reduces, that’s usually a favorable response pattern.
From the Clinic: Dr. Arora’s Expert Insight
The most common reason body leaning to one side lower back pain drags on is that people skip the clinical sequence. They see press-ups online and try them immediately—while the shift is still present. In real patients with a visible lateral shift, extension before correction often produces a sharp block or sends symptoms further down the leg. When I follow the correct order—shift correction first, then extension to “lock in” the change—patients usually regain midline faster and flare less. The posture is often protective; you don’t win by forcing it straight. You win by restoring alignment in the direction the spine will tolerate, then reinforcing it with the right loading progression.
Fixes: the correct order of operations (critical)
If you have a visible fixed lateral shift, treat your pain like this: body leaning to one side lower back pain
Plan A (must come first): Correct the shift
Your first job is to realign the pelvis under the ribcage.
Only when you are closer to midline should you move to Plan B.
Plan B (only after Plan A improves alignment): Extension to reinforce
Press-ups (or extension loading) are often used after the shift reduces, to help maintain/restore normal mechanics—especially in disc-sensitive patterns.
If Plan A does not improve alignment at all, or if symptoms rapidly peripheralize, stop and get assessed.
Plan A: Side-glide correction
Step 1: Identify your shift direction
- If your shoulders are shifted to the RIGHT of your pelvis, you have a right shift
- If your shoulders are shifted to the LEFT, you have a left shift
Step 2: Wall setup (the simplest self-correction)
Rule: Stand with the side you are leaning toward against the wall.
If you have a RIGHT shift (shoulders right of hips)
1.Stand beside the wall with your right side closest to it (body parallel to the wall).
2. Lightly touch the wall with your right shoulder/upper arm only (left shoulder stays away).
3. Keep both feet 20–30 cm away from the wall, still parallel and facing forward.
4. Keeping your right shoulder in contact and your chest facing forward, slide your pelvis to the right (toward the wall) so your hips move under your ribcage.
Return only a little (don’t bounce), and repeat.
Dose: 10 reps × 2–3 rounds/day, as tolerated.
One-line “anti-confusion” cue
✅ Only ONE shoulder touches the wall.
✅ Your chest faces forward.
✅ Your pelvis is what glides sideways.

Treatment for body leaning to one side lower back pain
Extra safety add-on (very important)
Stop and reassess if:
- leg pain travels further down (peripheralization),
- new tingling/numbness starts,
- pain becomes sharp/electric with each rep.
If you have a LEFT shift (shoulders left of hips)
Same steps, but mirror them:
- left shoulder to wall
- pull hips toward the wall (to the left)
Dose: 10 reps, rest 30–60 seconds, repeat 2–3 rounds/day.
What should it feel like?
- You may feel a firm stretch or pressure, but it should not create a new “electric” leg pain.
- Best sign: after a set, you look a bit more centered and/or symptoms move upward.
Stop immediately if
- pain spreads further down the leg (peripheralization)
- new numbness/tingling starts
- you feel unstable or faint
(This sequence aligns with clinical descriptions of lateral shift management in MDT-style case care: shift correction → self-management → rehab progression.)
Plan B: Press-ups (only after the shift is reduced)
Once you are closer to midline (even 30–50% improvement), you can trial gentle extension to reinforce the correction.
Prone on elbows (entry level)

Treatment for body leaning to one side lower back pain
- Lie on stomach
- Prop on elbows
- Hold 30–60 seconds, slow breathing
Small press-ups (progression)

Treatment for body leaning to one side lower back pain
- Hands under shoulders
- Press up gently while hips stay down
- Stop before sharp block or leg symptom spread
Dose: 8–10 reps, 1–3 sets/day if tolerated.
Rule: If press-ups worsen leg symptoms, stop and return to Plan A or relief positions.
First 72 hours: what to do and what to avoid
Do
- short frequent walks (5–10 minutes, 3–6x/day)
- relief positions (side-lying with pillow; or on back with calves supported)
- heat or ice (10–15 minutes, whichever helps)
Don’t
- force yourself straight for long periods
- stretch aggressively into pain
- twist/crack to “put it back”
- load carries early while the disc is irritable
Rehab plan (safer timeline for a lateral shift pattern)
A visible lateral shift implies high sensitivity. Week 2 should emphasize symptom control + endurance + symmetrical stability, not lateral shear loading.
Week 1: calm + control
1) 90/90 breathing with gentle brace
5 breaths × 3 rounds/day
2) Glute bridge
8–12 reps × 2 sets
3) Side plank (modified, knees)
10–20 seconds × 3 holds/side
4) Short walks
Most days, frequent and brief
Week 2: stability endurance (no lateral shear)
5) Dead bug (slow, controlled)
- Keep ribs down, low back quiet
- Alternate arms/legs without arching
6–8 reps/side × 2 sets
6) Bird dog (slow)
6–8 reps/side × 2 sets
7) Hip hinge drill (pattern only, no load)
8–10 reps × 2 sets
Week 3–4: symmetrical loading and tolerance
- increase walking duration gradually
- add light bilateral resistance (symmetrical) as tolerated
- continue dead bug/bird dog/bridge progressions
Week 4–6: carries (only if stable and symptom-free with basics)
Suitcase carry (single weight) — introduced later
Because it challenges lateral stability and can increase lateral shear, it fits better once the system is calmer and endurance is rebuilt.
Start light:
- 20–30 steps each side × 2–3 rounds
Stop if symptoms return or posture shifts.
(If you want a safer carry earlier, keep it symmetrical—two light weights—after Week 3 if symptoms are stable.)
Myths vs facts
Myth: “Any lean means SI joint problem.”
Fact: SI/hip pain more often causes a walking limp/antalgic lean, not a fixed trunk list while standing still.
Myth: “Press-ups are always step one.”
Fact: With a visible lateral shift, shift correction usually comes first. Extension before correction can worsen leg symptoms.
Myth: “If I’m crooked, my spine is permanently out of place.”
Fact: Most cases are temporary protective patterns that improve with the correct sequence and loading progression.
When to see a clinician
Get evaluated if body leaning to one side lower back pain:
- does not improve in 7–10 days
- repeatedly returns with minor triggers
- includes worsening numbness/weakness
- prevents normal walking/sleep
- peripheralizes with gentle correction attempts
Ask for: neuro screen + directional preference testing + shift correction strategy + staged rehab plan.
FAQ
1) Why does body leaning to one side lower back pain happen suddenly?
Often due to acute disc/nerve sensitivity leading to a protective lateral shift. Muscle guarding can contribute, but a fixed trunk list is a key clue.
2) Is body leaning to one side lower back pain always a disc problem?
Not always, but a fixed lateral shift pattern is strongly suggestive of disc/nerve irritation compared to SI-only pain.
3) Should I try press-ups immediately?
Not if you have a visible shift. Use Plan A first (side-glide correction). Press-ups are Plan B after alignment improves. in cases of body leaning to one side lower back pain first always fix the shift.
4) What’s the biggest sign I’m doing the right exercise?
in cases of body leaning to one side lower back pain if symptoms centralize (move upward toward the back) or your posture becomes visibly more centered without leg symptom spread.
5) What if side-glides increase pain down my leg?
If your body leaning to one side lower back pain and pain goes down lo legs after exercise Stop Immediately. That’s peripheralization. Return to relief positions and get assessed.
6) Is walking good for body leaning to one side lower back pain?
Usually yes, but keep it short and frequent. Stop if symptoms spread further down the leg.
7) Heat or ice? If body leaning to one side lower back pain.
Choose what reduces symptoms. Either can be useful for short sessions (10–15 minutes).
8) Can massage fix a lateral shift?
In Cases of body leaning to one side lower back pain massage may reduce guarding temporarily, but true shift correction usually requires direction-specific repositioning plus a rehab progression.
9) When do I start strengthening?
In body leaning to one side lower back pain Once the shift is improving and symptoms are calmer. Week 1–2 = stability endurance; heavier/lateral loading later.
10) When is it an emergency?
Bowel/bladder changes, saddle numbness, progressive weakness, fever/systemic illness, major trauma with body leaning to one side lower back pain—seek urgent evaluation.