Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.
One moment you feel the familiar build-up — that tickle at the back of the nose. Before you can brace yourself, a sneeze fires through your body and sends a sharp, shooting pain into your lower back. For a second, you freeze.
Sharp pain in the lower back when sneezing is one of the most common complaints I have seen in clinical practice. And while it sounds alarming — because sudden spinal pain never feels like good news — the cause is almost always mechanical, not catastrophic. That said, context matters enormously. Understanding what is actually happening inside your lumbar spine during a sneeze goes a long way toward knowing whether this is something to manage at home or something that needs proper assessment.
Let us work through this properly.

Key Takeaways
- A sneeze creates a sudden burst of pressure and forceful trunk bracing — if a spinal structure is already irritated, that pressure spike can light it up immediately.
- The most common culprits are lumbar muscle spasm, disc irritation or herniation, facet joint irritation, and sacroiliac region sensitivity — not always the dramatic “slipped disc” people fear.
- If sneezing also shoots pain down the leg, adds numbness, or causes weakness, a nerve-root or disc-related pattern becomes more concerning and should be assessed.
- Most people do not need immediate imaging just because sneezing hurts.
- Seek urgent care if pain comes with loss of bladder or bowel control, saddle-area numbness, rapidly worsening leg weakness, fever, significant trauma, or unrelenting pain unaffected by position.
What Causes Sharp Pain in Lower Back When Sneezing?
Sharp lower back pain when sneezing usually happens because a sneeze creates a sudden pressure spike and forceful trunk brace that irritates an already sensitive structure in the low back. The most common sources are a lumbar disc, back muscle spasm, facet joint irritation, or tissues around the sacroiliac region.
- If pain stays mostly in the lower back, it is more often mechanical and local.
- If pain shoots into the buttock or leg, a disc or nerve-root pattern becomes more likely.
- If pain comes with numbness, weakness, or bladder/bowel changes, it needs urgent medical assessment.
The Mechanics: Why a Sneeze Can Hurt the Lower Back
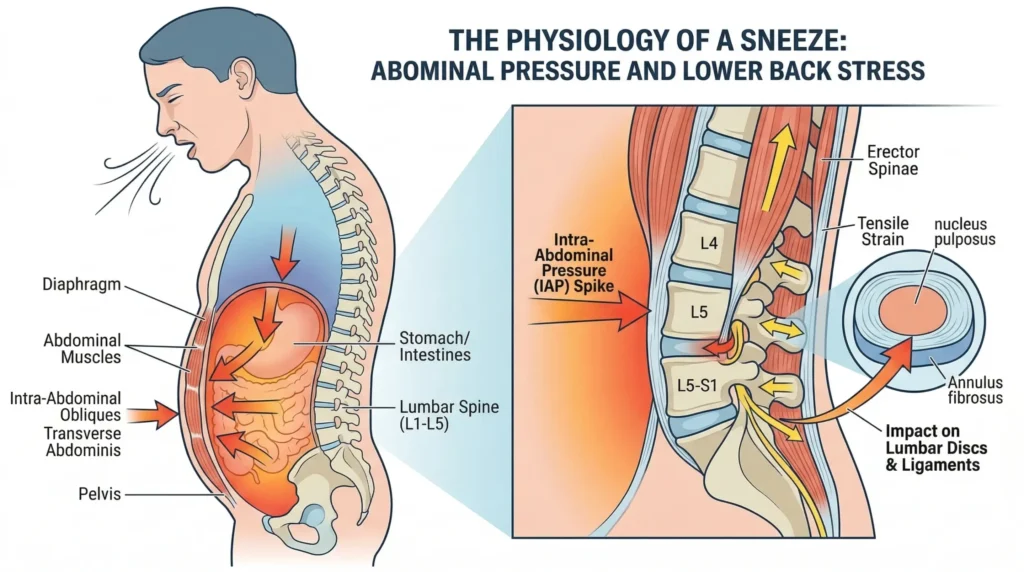
A sneeze is not a small event, mechanically speaking. In the fraction of a second before air is expelled, your body performs something close to a Valsalva maneuver — you inhale sharply, close the glottis, and powerfully contract your abdominal, chest, and trunk muscles simultaneously. The pressure inside your chest and abdominal cavity spikes dramatically.
Research measuring intradiscal pressure in the lumbar spine has shown that activities involving sudden trunk loading — including coughing and sneezing — generate some of the highest compressive forces the lumbar discs experience, comparable to or exceeding those produced during many lifting tasks.¹ If structures in your lower back are already irritated, inflamed, or structurally compromised in some way, that sudden pressure surge can feel like someone driving a spike into the base of your spine.
The jolt also catches the paraspinal muscles off guard. These muscles — particularly the erector spinae and multifidus — are designed to stabilize the spine through anticipated movement. A sneeze is often unanticipated. The muscles cannot pre-tension in time, leaving the passive structures — discs, ligaments, joints — to absorb the load largely unprotected.
That does not automatically mean something tore. Often it means one tissue has temporarily lost its load tolerance, and the sneeze simply exposed it. This is the same principle behind why low back pain occurs in everyday situations — cumulative stress building quietly until a single event triggers it.
The 4 Most Common Causes of Sharp Lower Back Pain When Sneezing
1. Disc Irritation or Disc Herniation
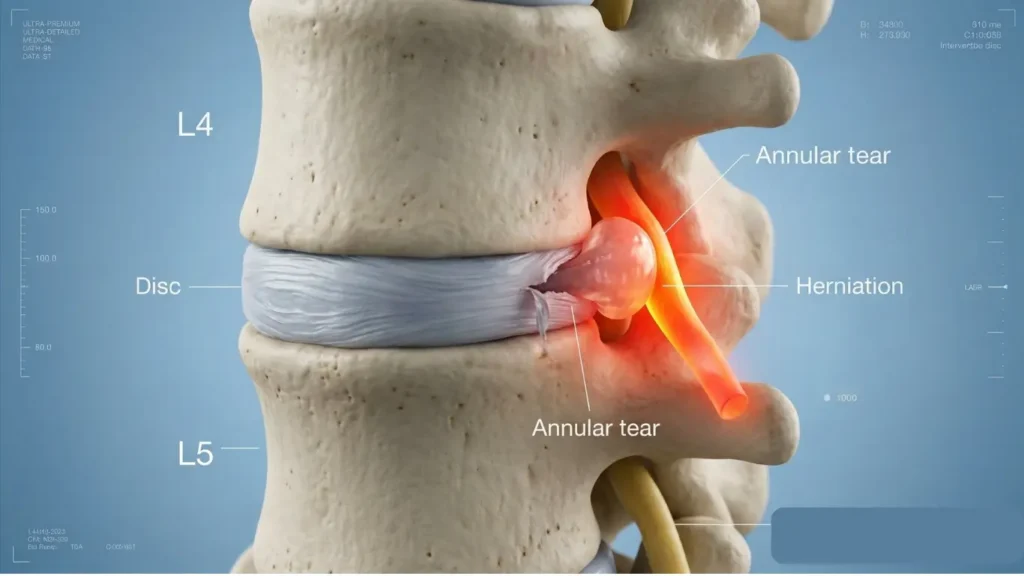
A lumbar disc is one of the first suspects when sneezing hurts, especially if the pain radiates into the buttock or leg. The intervertebral discs are gel-filled cushions sitting between each vertebra. When a disc is herniated — meaning its inner nucleus has pushed through the outer fibrous ring — the surrounding tissue is already sensitized and inflamed. A sneeze-driven pressure surge can trigger a sudden, intense flare.
Worth noting: not every disc issue that hurts with a sneeze is a frank herniation. Annular tears — small fissures in the outer disc wall — can be acutely sensitive to pressure changes and produce significant pain without any disc material directly pressing on a nerve. In patients with sciatica, worsening leg pain during coughing, sneezing, or straining carries significant diagnostic value for nerve-root compression and disc herniation on MRI.²
Typical clues:
- Pain shoots into the buttock, thigh, calf, or foot
- Sitting feels worse than walking
- You may feel tingling, numbness, or a sense of weakness
- Bending forward, putting on socks, or getting out of a car may also provoke it
2. Acute Muscle Spasm or Strain
This is the most common culprit. The paraspinal muscles can be in a low-grade state of tension from lifting something awkward, poor sleep position, long hours of sitting, or cumulative daily load. The sudden explosive contraction triggered by a sneeze can push an already irritated muscle into full spasm, producing a sharp, seizing pain that typically stays local to the lower back.
The intensity can be genuinely surprising. People often describe it as a “catch” or a “locking” sensation. What is happening is protective — the muscle contracts to guard the area — but that contraction is itself painful.
Typical clues:
- Pain is mostly in one local spot — a “catch” or “locking” sensation
- It hurts to straighten up after bending
- There is no clear numbness or tingling down the leg
- Coughing, laughing, rolling in bed, or standing from a chair may also provoke it
3. Facet Joint Irritation
The facet joints are small, pain-sensitive joints at the back of each vertebral segment. They guide spinal movement, share compressive load, and are richly supplied with nerve endings. When they are irritated — through prolonged postural load, degeneration, or a slight sprain — the sudden trunk pressure of a sneeze can provoke a sharp, localized catch, often felt more to one side than the other.
Facet-related pain tends to be worse with extension and rotation and rarely causes true neurological symptoms below the knee.
Typical clues:
- Pain stays more in the back than the leg
- Worse when standing upright after sitting, or when twisting and turning in bed
- Leaning backward can reproduce it
4. Sacroiliac (SI) Joint Dysfunction
The SI joint sits at the junction of the lower spine and pelvis. Dysfunction here — from hypermobility, joint degeneration, or pregnancy-related ligament laxity — can produce a sharp, stabbing pain near the “dimple” area at the base of the spine when load suddenly transfers through the pelvis. Sneezing is precisely that kind of sudden load event. If you notice the pain specifically near the lower back dimples, the SI region is a strong candidate.
SI joint pain is usually unilateral and may refer into the groin or upper thigh, but rarely travels below the knee in a true nerve-root pattern.
Typical clues:
- One-sided pain low and slightly off-center near the dimple area
- Pain when standing on one leg, climbing stairs, or rolling over in bed
- Tenderness near the back of the pelvis rather than the center of the spine
5. Less Common Non-Spine Causes
Not every pain felt in the low back starts in the spine. Kidney stones, abdominal causes, and hip-related problems can occasionally mimic back pain — particularly if the pain pattern is unusual, colicky, or associated with urinary symptoms, fever, or a rash. That becomes more relevant when the pain is not clearly linked to movement or position.
How to Tell Which Pattern You May Have
A useful first question is: Is it just back pain, or back pain plus leg symptoms?
| Symptom Pattern | Most Likely Source |
|---|---|
| Localized, sharp, no numbness or tingling | Muscle or facet irritation |
| Back pain plus buttock or leg pain, especially below the knee | Disc or nerve-root pattern |
| One-sided near the dimple, pain on single-leg loading or turning | Posterior pelvic / SI region |
| Pain in both legs simultaneously with numbness or weakness | Urgent — see red flags below |
| Constant, unrelenting, position-independent | Non-mechanical cause — requires assessment |
Another useful clue is how the pain behaves over 24 to 72 hours. Mechanical pain typically changes with position, movement, or load. Serious pathology tends to look relentless, progressive, or is accompanied by systemic symptoms.
Red Flags: When to Seek Immediate Medical Attention

Most sneezing-related back pain is a mechanical event in an otherwise recoverable spine. However, certain symptoms require urgent or emergency medical care:
- New trouble controlling bladder or bowel function — difficulty urinating or incontinence may indicate cauda equina syndrome, a medical emergency
- Numbness in the groin, genitals, or inner thighs — often called “saddle area” numbness
- Rapidly worsening or bilateral (both sides) leg weakness
- Major trauma — a fall, road accident, or direct impact to the spine
- Unexplained weight loss, fever, chills, or night sweats alongside back pain
- Known or suspected history of cancer — any new or persistent back pain warrants prompt assessment
- Pain that is constant, unrelenting, and completely unaffected by position or movement
If any of these features are present, do not attempt home management. Seek emergency or urgent medical care promptly.
Do You Need an MRI or X-Ray Right Away?
Usually, no.
In most cases of acute lower back pain triggered by sneezing, imaging in the first few weeks is unlikely to change management. Current clinical guidelines — including the NICE guideline on low back pain and sciatica — explicitly advise against routine imaging for non-specific presentations without red flags.³ The full explanation of what a low back pain X-ray or MRI can and cannot tell you is worth reading before requesting one.
The reason matters: MRI findings in the lumbar spine, such as disc bulges, mild herniations, and age-related degenerative changes, are extremely common in adults who have no back pain at all. Treating an image rather than a patient leads to unnecessary anxiety, over-medicalization, and often unnecessary intervention. Pain intensity alone does not equal imaging urgency.
Imaging becomes appropriate when:
- Red flags are present
- Neurological deficit is progressive — worsening leg weakness or expanding numbness
- Conservative treatment has failed after 4–6 weeks and the diagnosis remains genuinely uncertain
- Surgical or invasive intervention is being considered
Myths Worth Clearing Up
“If sneezing hurts, it must be a slipped disc.” Discs do not actually “slip.” They can bulge, herniate, or degenerate — and even then, a single sneeze is rarely the primary cause of a new herniation. More often, a disc that was already under stress gets pushed past its tolerance threshold. The sneeze reveals the problem; it usually did not create it.
“If the pain is sharp, something must have torn.” Sharp does not always mean torn. Acute muscle spasm alone can be agonizing and yet resolve completely within days. Pain intensity is a poor predictor of tissue damage in the lumbar spine. Red flags, not pain severity, determine whether something is serious.
“Bed rest is the fastest fix.” Prolonged bed rest has been consistently shown to slow recovery and worsen outcomes.⁴ Gentle movement within pain tolerance is part of the treatment from early on — not the exception.
“An MRI will tell me exactly why it hurts.” Sometimes it helps, but not always. Imaging findings can be useful in the right context, but they still have to match your symptoms and clinical examination. Many findings on MRI — disc bulges, degenerative changes, minor herniations — are common in people with no pain at all.
From the Clinic: Dr. Arora’s Expert Insight
There is a pattern I have seen repeatedly, and I think it is worth naming directly: people arrive after a sneeze-triggered episode convinced they have caused a catastrophic injury. By the time I see them, they have spent several days flat on their back waiting for the damage to declare itself. The muscle guarding that started as a protective response has now compounded the original problem, the joints have stiffened from disuse, and the fear of movement has set up a cycle that is harder to break than the original pain.⁵
Here is what I have come to understand: the sneeze is almost never the villain. It is more like a stress test. It exposes a spine that was already working harder than it should — because of prolonged sitting, a movement habit that distributes load poorly, a previous injury that was never fully rehabilitated, or cumulative disc stress that had been quietly building. The sneeze is the moment that makes the problem impossible to ignore.
The other thing worth discussing practically is sneeze technique — which almost no one thinks about until they are in pain. If your back is currently sensitive, sneezing with a relaxed, unsupported trunk is essentially letting a pressure wave hit an unbraced wall. The simple act of bending slightly at the knees, lightly bracing your abdominals, keeping your chin slightly tucked toward your chest, and supporting yourself with one hand on a nearby surface when you feel a sneeze coming can meaningfully reduce the load through the lumbar structures. It sounds almost embarrassingly simple, but I have seen it make a genuine difference in acute episodes.
The third thing I would offer is perspective on prognosis: do not judge your spine by a single dramatic event. Some of the most alarming-sounding sneeze stories I have heard — sharp pain, could not move for several minutes, feared the worst — turned out to be straightforward muscular episodes that responded beautifully to a week of appropriate movement, manual therapy, and sensible load management. The sharp presentation rarely predicts a long or complicated recovery.
Instant Relief: What to Do in the First 24 to 72 Hours
There is no universal magic trick, but these steps help most people reduce pain spikes quickly. The same principles apply whether the trigger was a sneeze or coughing with lower back pain, since both events create the same sudden trunk pressure surge.
1. Use a “Supported Sneeze” Strategy

If you feel a sneeze building:
- Bend slightly at the knees
- Gently brace your abdominals
- Place one hand on a wall, desk, or your thighs
- Keep your chin slightly tucked toward your chest as the sneeze fires — this reduces spinal load compared to sneezing with the neck extended or thrown back
This becomes instinctive with a little practice during the acute phase.
2. Find the Least-Irritating Position
Some people get relief lying on their back with knees bent and feet flat on the surface. Others prefer side-lying with a pillow between the knees. Use this position to let the acute pain settle — but do not stay there all day.
3. Apply Heat or Ice
Both can help, and personal preference matters. Ice (15–20 minutes with a cloth barrier) may be useful in the first 24–48 hours if there is a sensation of local heat or acute inflammation. Heat — a warm pack, hot water bottle, or warm bath — tends to work better for muscle spasm. Use whichever leaves you moving better afterward.
4. Reduce the Spike, Not All Movement
You do not need total rest. Avoid repeated bending, twisting, and heavy lifting for a day or two, but take short, gentle walks to prevent the spine from stiffening up completely.
A Phase-Based Rehab Progression
A good rehab plan does not just reduce pain — it reduces how easily pain is triggered again. For a comprehensive home exercise programme, the low back pain exercises physical therapy guide provides step-by-step instructions alongside the phase framework below.
Phase 1 — Acute (Days 1–5): Calm It Down
Goal: Reduce pain spikes and get out of the “every sneeze feels dangerous” stage.
Focus on short walks, comfortable position changes, easy core bracing without breath-holding, and gentle lumbar or hip motions that do not worsen symptoms. Pelvic tilts and slow single-knee-to-chest stretches are appropriate here. Over-the-counter pain relief — paracetamol or anti-inflammatories if appropriate and not contraindicated — can help manage pain sufficiently to allow gentle movement.
Phase 2 — Subacute (Days 5–14): Restore Movement
Goal: Stop the back from depending on one guarded, stiff pattern.
Introduce hip hinge retraining, rolling in bed without twisting, sit-to-stand control, gentle cat-cow mobility, and early bridge exercises for gluteal and lumbar activation. Movement should feel productive, not provoked.
Phase 3 — Recovery (Weeks 2–6): Rebuild Load Tolerance
Goal: Return to normal daily life without the back overreacting to ordinary stress.
Progress to controlled bending, split-stance loading, bird-dog and dead bug variations, and glute and trunk endurance work.⁶ The spine needs to learn to handle load again — not be protected from it indefinitely. Hip and glute strength are frequently overlooked contributors at this stage and are worth addressing alongside lumbar work.
Phase 4 — Return to Full Activity: Reload What Matters
Goal: Gradual re-exposure to sport, gym training, sustained postures, or heavy occupational tasks with attention to form and load progression.
This is also the right time to address whatever predisposed the spine in the first place — hip strength deficits, core stability, workstation setup, or ingrained movement habits. Resolving the episode is one goal; reducing the likelihood of the next one is the other.
Do’s and Don’ts
Do:
- Keep moving gently and regularly within your pain tolerance
- Support yourself (bend knees, brace, tuck chin) before coughing or sneezing
- Use heat for muscle spasm and ice for acute focal inflammation
- Pay close attention to whether pain travels below your knee
- Seek a physiotherapy assessment if pain is not meaningfully improving within 5–7 days
Don’t:
- Rest completely in bed for days on end — it prolongs recovery
- Keep “poking the bruise” by repeatedly testing painful bending movements
- Assume the worst because the pain was sharp
- Ignore red flag symptoms like saddle numbness or bladder changes
- Rush back into heavy lifting, running, or contact sport before pain has fully resolved
- Over-rely on imaging to guide every decision — it frequently creates more anxiety than clinical clarity
When Conservative Care Is Not Enough
Consider a formal assessment by a physical therapist, primary-care clinician, or spine specialist if:
- Symptoms are not clearly improving within 4–6 weeks
- Leg pain is becoming more dominant than back pain
- Numbness or weakness is appearing or progressing
- Repeated sneezing, coughing, sitting, or bending keep reproducing the same flare
- Pain keeps returning every few weeks
Interventions such as nerve root injections or epidural steroid injections may be appropriate for persistent and significant radicular pain that has not responded to conservative care.
Surgery is rarely indicated for acute lower back pain triggered by sneezing. When it is considered, it is typically for confirmed disc herniation with progressive neurological deficit or cauda equina syndrome, which remains a surgical emergency.
Outlook: Should You Worry?
The majority of acute lower back pain episodes — including those triggered by sneezing — follow a favorable natural course. Most people experience significant improvement within two to four weeks. A proportion will have residual sensitivity or occasional flares, particularly if the underlying issue — disc irritation, movement habit, deconditioning — is not properly addressed as part of recovery.
The important question is not whether the sneeze hurt. It is what pattern the sneeze revealed. If pain is mainly local, mechanical, and gradually calming, the outlook is usually good with smart load management and progressive rehab. If sneezing repeatedly worsens leg pain, numbness, or weakness, or red flags are present, that is the point to escalate — promptly.
Conclusion
Sharp pain in the lower back when sneezing is a startling, uncomfortable experience — and an understandably worrying one when it happens without warning. In the vast majority of cases, however, it reflects a mechanical response in a spine that was already under some degree of stress, not a catastrophic new injury caused by the sneeze itself.
The causes range from lumbar muscle spasm and facet joint irritation to disc involvement, and distinguishing between them requires a proper clinical assessment when pain persists or when neurological symptoms are present. Red flags — particularly loss of bladder or bowel control, bilateral leg weakness, or saddle area numbness — require immediate medical attention without delay.
For most people, the path forward involves early gentle movement, sensible load management, targeted rehabilitation, and a better understanding of how to protect the spine during high-pressure events — including, yes, the humble sneeze.
Frequently Asked Questions
1. Can sneezing really cause sharp lower back pain?
Yes. Sneezing can trigger sharp lower back pain because it creates a sudden burst of pressure and muscle bracing through the trunk — similar in mechanism to a Valsalva maneuver. That force often exposes an already irritated disc, muscle, facet joint, or sacroiliac-region tissue rather than creating a brand-new injury. For a broader overview, see what causes lower back pain and how cumulative stress sets the stage.
2. Is sharp lower back pain when sneezing a slipped disc?
Not always. A disc is one possibility, but muscle spasm, facet joint irritation, and SI joint sensitivity can all react just as sharply. If sneezing also makes pain shoot into the buttock or leg, a disc or nerve-root pattern becomes more likely and warrants clinical assessment.
3. Why does my back hurt when I sneeze but not all the time?
Usually because the sneeze briefly overloads a sensitive structure that is calm at rest but reactive under sudden pressure. That is common with early disc irritation, muscle spasm, facet irritation, or a stiff, overloaded low back that has accumulated stress over time.
4. When should I worry about lower back pain when sneezing?
You should seek urgent care if the pain comes with leg weakness, numbness, saddle-area numbness, bladder or bowel changes, fever, major trauma, or unrelenting pain that does not behave like a normal mechanical flare. Those patterns need prompt medical review — they are not “watch and wait” situations.
5. Should I go to the ER if I feel a “snap” or jolt in my back when I sneeze?
A “snap” in this context is almost always a sensation, not evidence of structural failure. Seek emergency care if you experience loss of bladder or bowel control, numbness around the inner thighs or groin, weakness in both legs, or if the pain follows significant trauma. Sharp back pain alone — without these features — does not typically require emergency attendance.
6. Should I rest or keep walking if sneezing hurts my lower back?
Keep moving gently unless movement clearly worsens the pain. Short walks and easy position changes are usually better than strict bed rest. Avoid repeated bending, twisting, and heavy lifting during the first one to two days, but do not become immobile.
7. Do I need an MRI if sneezing causes back pain?
Usually not right away. Most people with mechanical low-back pain do not need immediate imaging unless red flags are present, neurological symptoms are progressing, or the diagnosis remains uncertain after a proper clinical assessment.
8. How long will lower back pain from sneezing take to resolve?
Most acute episodes settle meaningfully within a few days to two weeks with gentle movement and load management. If significant pain persists beyond three to four weeks, or if leg symptoms are present, a clinical assessment and potentially imaging are appropriate.
Medical Disclaimer
This article is intended for general informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment. The content reflects the clinical experience and perspective of the author and should not replace consultation with a qualified healthcare professional. If you are experiencing back pain accompanied by neurological symptoms, loss of bladder or bowel control, or any of the red flags described in this article, seek immediate medical attention. Always consult a licensed physician or physical therapist for assessment and management specific to your situation.
References
- Nachemson AL. Disc pressure measurements. Spine (Phila Pa 1976). 1981;6(1):93–97. PMID: 7280086.
- Verwoerd AJH, Mens J, El Barzouhi A, Peul WC, Koes BW, Verhagen AP. A diagnostic study in patients with sciatica establishing the importance of localization of worsening of pain during coughing, sneezing and straining to assess nerve root compression on MRI. European Spine Journal. 2016;25(5):1389–1392. doi:10.1007/s00586-016-4393-8.
- National Institute for Health and Care Excellence (NICE). Low back pain and sciatica in over 16s: assessment and management. NICE guideline [NG59]. Published December 2016; updated 2020. Available at: https://www.nice.org.uk/guidance/ng59
- Hagen KB, Hilde G, Jamtvedt G, Winnem MF. The Cochrane review of advice to stay active as a single treatment for low back pain and sciatica. Spine. 2002;27(16):1736–1741. doi:10.1097/00007632-200208150-00013.
- Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–332. doi:10.1016/S0304-3959(99)00242-0.
- Hides JA, Jull GA, Richardson CA. Long-term effects of specific stabilizing exercises for first-episode low back pain. Spine. 2001;26(11):E243–E248. doi:10.1097/00007632-200106010-00004.