Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.
Few home-care questions arrive in clinical practice with as much confident misinformation attached as this one. Half the internet says ice. The other half says heat. Both sides have a story, and neither is entirely wrong — which is part of why the debate refuses to die.
Here is the part that actually matters: the answer is not universal. Whether to use ice or heat for lower back pain depends on what is happening in your specific tissues at that specific moment. Pick the wrong one and you either accomplish nothing or — in a meaningful number of cases — make things worse. Pick the right one and you reduce pain, restore movement, and give your body the environment it needs to start recovering.
This guide works through the physiology, the clinical scenarios, the practical application rules, and the situations where neither modality is the real answer.
Key Takeaways
- Heat is the better choice for most lower back pain — muscle tension, morning stiffness, subacute or chronic presentations.
- Ice has a specific role in the first 24–48 hours of a traumatic injury with visible signs of tissue damage or swelling.
- Most common lower back pain — including the familiar flare after a bad lift or a long day at a desk — involves muscle guarding and restricted circulation, not active bleeding. Cold makes that worse.
- Both are symptom managers. Neither addresses the underlying mechanical cause.
- Radiating leg pain, numbness, bladder or bowel changes, fever, or pain following trauma require clinical evaluation — not a temperature decision.

Ice or Heat for Lower Back Pain: The Quick Clinical Answer
For most lower back pain, heat is the better choice. It improves circulation, reduces muscle spasm, and directly addresses the tissue state that drives the majority of lumbar pain presentations. Ice is appropriate in a narrower window: the first 24 to 48 hours of a clearly traumatic injury where acute inflammation and tissue damage are present. When in doubt about which applies to your situation, heat is the safer default for non-traumatic back pain.
What Cold and Heat Actually Do to Tissue
The popular explanations for both modalities tend to flatten the physiology in ways that cause people to make the wrong choice. Here is what is actually happening.
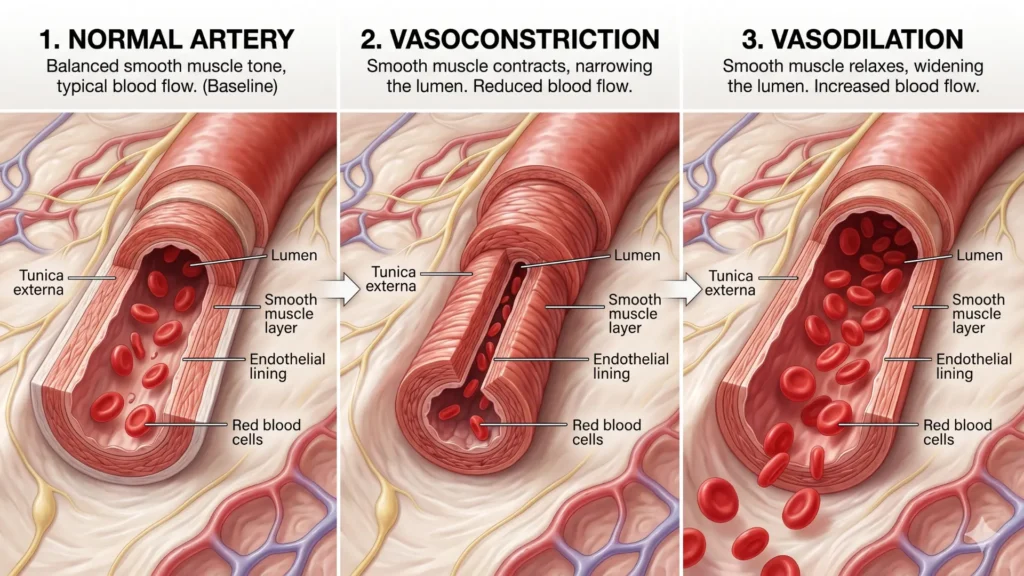
Cold application causes vasoconstriction — the blood vessels directly beneath the skin contract, reducing local circulation. Tissue temperature drops, which slows nerve conduction velocity: pain signals travel more slowly and fire less frequently. Cold also suppresses the early-phase enzymatic activity associated with acute inflammation. In a freshly injured tissue — a torn muscle fiber, a sprained ligament, a bruised joint — that cascade is genuinely useful. Slowing it down in the first 24 to 48 hours limits secondary tissue damage and reduces swelling.
Heat application does the opposite. Vasodilation follows, drawing more blood into the area. Increased circulation clears metabolic waste products — primarily lactic acid and inflammatory byproducts that accumulate in chronically contracted or poorly perfused muscle. Heat also directly reduces stiffness in collagen-rich soft tissues, allowing them to lengthen and move more freely. Simultaneously, thermoreceptors in the skin send competing signals to the spinal cord, partially gating out pain signals through a mechanism sometimes called counter-irritation. The result is less perceived pain, reduced spasm, and improved range of motion.
The clinical implication is precise: cold addresses active bleeding and acute inflammation. Heat addresses ischemia, guarding, and restricted blood flow. These are different tissue states, and understanding which one you have is the entire basis for the ice-or-heat decision.
Why the Lower Back Responds Differently to Cold Than Other Body Parts
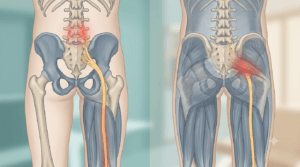
The lumbar spine is surrounded by a dense architecture of overlapping muscles. The erector spinae columns run vertically alongside the vertebral bodies. The multifidus — arguably the most functionally important of the group — sits in close contact with individual spinal segments and acts as a real-time stabilizer with every movement. The quadratus lumborum bridges the lower ribs to the iliac crest and governs lateral stability. Beneath all of this, the thoracolumbar fascia connects the whole system into a tension network that responds to load, posture, and even psychological stress.
When any of these structures is threatened — by a loaded movement, by sustained compression from prolonged sitting, or by referred input from an irritated disc or facet joint — the response is protective spasm. The muscle contracts reflexively to limit further movement and guard the sensitive area. This is not pathology. It is the nervous system doing exactly what it is designed to do.
The problem is duration. Sustained muscle contraction compresses the capillaries running through the muscle tissue, reducing blood flow below the threshold needed to clear waste products. Pain builds. Sensitivity increases. The muscle contracts harder in response to the pain — and the cycle reinforces itself. This is ischemic pain: a deep, dull, worsening ache that typically feels better with the first few minutes of gentle movement and worse with sustained posture.
Apply ice to that state and the vasoconstriction reduces blood flow further. The ischemia deepens. The muscles respond to the temperature drop by contracting more — it is a reflex, not a choice. Most people who apply ice to guarding lumbar muscles for several days report feeling progressively stiffer, not better. This is not coincidence. It is the predictable physiological response to applying a vasoconstrictor to an already underperfused tissue.
Apply heat, and the opposite sequence unfolds.
When Ice Does Make Clinical Sense for Lower Back Pain
Ice is not useless — it is just misapplied far more often than it is applied correctly.
Acute traumatic injury in the first 48 hours: A fall, a direct blow, a sudden muscular tear with visible bruising or swelling — these are presentations where active inflammatory processes and tissue bleeding are present, and cold application is appropriate. The key markers are sudden-onset pain following a specific incident, swelling or bruising at the affected area, and pain that worsens rapidly with movement in the first hours. Outside this window, most of the rationale for ice evaporates.
Post-exercise soreness in the lumbar region: If you have returned to heavy training after a break and your lower back is sore following a loaded session — deadlifts, barbell rows, heavy carries — brief cold application may reduce the intensity of delayed-onset muscle soreness. This is a different tissue state from mechanical back pain, and ice is reasonable here.
Very acute disc flares with significant nerve irritation: Some clinicians recommend brief cold application in the first 24 to 48 hours of a sudden disc-related flare, particularly when there is significant nerve root irritation and heat feels intolerable. The rationale is limiting local neurogenic inflammation acutely. This is not well-established in the evidence and individual responses vary considerably — if cold consistently increases your leg symptoms or worsens the spasm, stop.
The Cochrane review of superficial heat and cold for low back pain found the evidence for cold therapy specifically to be insufficient to draw firm conclusions, with conflicting data on whether it offers any advantage over heat for lower back outcomes. That finding has not substantially shifted since publication. Ice may help some people in the acute traumatic phase; beyond that window, its role is limited.
When Heat Is the Right Call
Heat covers the large clinical middle ground: most of what people actually experience as lower back pain.
Morning stiffness: The lumbar spine goes through a predictable process overnight. Sustained positional loading and relative immobility lead to fluid redistribution, mild disc swelling, and the kind of muscular stiffness that takes 20 to 30 minutes to work out. A warm shower or heat pack applied before movement is one of the most effective interventions for this pattern — it cuts the warm-up phase and reduces the pain that makes people avoid morning movement.
Subacute and chronic pain: Pain that has been present for more than a few days, or that returns in recognizable cycles, is almost never driven by acute inflammation. Tissues are irritable, circulation is poor, and protective guarding has become habitual. This is the territory heat was designed for.
Stress-related or postural loading pain: Sustained desk posture, long periods of driving, carrying children on one side — these load the lumbar musculature unevenly and chronically. The resulting tension responds well to heat, particularly when followed immediately by movement.
Muscle-dominant presentations: Pain that develops with sustained positions, worsens through a long workday or sitting stretch, eases briefly with position changes or short walks, and feels more like a persistent ache than a sharp, catching, or electric sensation — this is most consistent with a musculoligamentous or muscle-dominant presentation. Heat is appropriate across this entire category.
The same Cochrane review found moderate evidence that heat wrap therapy reduces both pain and disability in people with acute and subacute lower back pain over the short term — a finding that held across multiple trials and was not replicated for cold.
When Temperature Therapy Is the Wrong Question
There is a category of lower back pain where reaching for ice or heat delays the evaluation that is actually needed.
Pain radiating down one leg: If your lower back pain travels past the buttock and down the leg — especially below the knee, with tingling, numbness, or weakness — you have neural involvement. The source of the problem is nerve compression or irritation at the spinal level, and temperature applied to the back surface does not reach or affect that. It may temporarily reduce the muscular component, but it is not a management plan for lumbar radiculopathy. Formal assessment is warranted. Understanding the full spectrum of symptoms that can accompany this pattern is covered in detail in our article on the 10 most common low back pain symptoms.
Saddle area numbness or bilateral leg changes: Loss of sensation in the inner thighs and groin, along with any change in bladder or bowel function, is a clinical emergency. This pattern suggests cauda equina involvement — pressure on the nerve root bundle below the spinal cord — and requires emergency evaluation. Do not attempt to manage this with any home therapy.
Pain following trauma: A fall from height, a road traffic accident, or any significant direct force to the spine — particularly in someone over 50, with known osteoporosis, or on long-term corticosteroids — requires imaging before physical therapy begins. A plain X-ray is typically the first-line investigation to rule out vertebral fracture. Heat or ice applied over an undiagnosed fracture is not dangerous in itself, but it distracts from the actual clinical priority.
Fever combined with back pain: Fever in the presence of back pain raises the possibility of spinal infection (discitis or osteomyelitis) — rare but serious and requiring urgent medical assessment, not conservative management. This combination should never be managed with home therapy alone.
Unexplained weight loss with persistent back pain: In anyone over 50, in anyone with a prior history of cancer, or in anyone whose back pain is progressive, night-dominant, and does not follow the mechanical pattern described above, imaging is appropriate. An MRI is typically more informative than X-ray for soft tissue pathology; a clinician will guide the decision based on the clinical picture. Understanding what is driving the pain is the starting point — and that assessment determines whether conservative care, imaging, or referral is the right path, as explored in our guide to what causes lower back pain and how to reset it.
From the Clinic: Dr. Arora’s Expert Insight
There’s a pattern that plays out in clinical practice with remarkable consistency: the patient who has been icing faithfully for five days is usually the stiffest one in the room. They’ve done exactly what they assumed was right — “injury means ice” — and they’re genuinely confused about why they feel worse with each passing day rather than better.
The misapplication almost always traces back to the same conceptual shortcut: treating lower back pain as a single category rather than as a tissue state. But “back pain” is not an indication for ice. It is not an indication for heat, either. What drives the decision is the underlying physiology — and in clinical practice, the single most useful question I ask is not “when did this start?” but “does moving around make the pain better or worse after the first five minutes?”
If gentle movement — a short walk, some slow pelvic tilts — reduces pain after an initial few minutes, the muscle-guarding pattern is dominant, and heat is almost certainly the right choice. If movement consistently and progressively worsens pain, especially with any leg component, that needs formal assessment. No temperature modality changes that answer.
The second pattern I see is people using heat correctly in the first week, feeling improvement, and then abandoning it the moment the pain becomes manageable. What they don’t realize is that the tissue state — tension, poor circulation, reduced movement — hasn’t fully resolved. The pain has dropped below the threshold of conscious discomfort, but the underlying problem is still present. The most effective use of heat in clinical practice is not passive: apply it for 15 to 20 minutes, then move. The window of reduced spasm that follows is when gentle rehabilitation — walking, mobilization exercises, early stability work — is most productive. Heat as a prelude to movement consistently outperforms heat as a substitute for it, and this combination is supported by the trial data.
Practical Application: How to Use Each Effectively
Ice: Application Guidelines
- Apply within the first 24–48 hours of a clearly traumatic injury where swelling or bruising is present.
- Always use a cloth barrier between the pack and skin — direct contact can cause ice burns within minutes.
- 15 to 20 minutes maximum per session; allow at least 45 to 60 minutes between applications.
- If leg symptoms worsen during or after application, stop immediately.
- Do not use cold on skin with reduced sensation — this includes areas affected by long-standing nerve compression or diabetic neuropathy.
- Skin temperature of around 10–15°C (50–59°F) at skin level is the therapeutic target; a thin cloth layer achieves this without risking burns.
Heat: Application Guidelines
- For non-traumatic lower back pain, heat is appropriate from the first episode onward (or after the initial 48-hour post-trauma window if applicable).
- 15 to 20 minutes per session; beyond this, vasodilatory benefit plateaus and skin irritation risk increases.
- Continuous low-level heat wraps — adhesive patches designed for 8-hour wear at around 40°C (104°F) — are well-supported in the evidence and practical for people who need relief during daily activity.
- Use heat before movement, not instead of it. The reduced spasm window is when rehabilitation is most effective.
- Do not sleep on an electric heating pad set to high. If overnight heat is needed, use heat wraps designed for that purpose.
- Avoid applying heat over significant bruising, open skin, or areas of acute trauma.
- Effective temperature range: 38–42°C (100–108°F) at skin level — warm enough to produce vasodilation without risking thermal damage.
Do’s and Don’ts
Do use a heat pack or warm shower before morning movement to shorten the stiffness period.
Do apply heat for 15–20 minutes before your prescribed exercises to reduce guarding and improve range of motion.
Do use ice within the first 48 hours of a traumatic injury if swelling or bruising is present.
Do keep moving gently after heat application — the goal is always to restore normal movement, not to extend the rest period.
Don’t apply ice to a stiff, guarding lower back that has been painful for several days without a traumatic incident.
Don’t treat heat as permission to stay still — its benefit is maximized when it precedes movement, not replaces it.
Don’t combine strong topical analgesic agents with a heating pad unless a clinician has advised this; the combination can produce skin reactions.
Don’t persist with either modality if it consistently worsens your pain — that response is information worth paying attention to.
Return to Activity: A Realistic Timeline
Temperature therapy has a defined role and a defined endpoint. The goal is to make movement possible — and movement is what produces durable recovery.
Days 1–3: Modify activity rather than stop it. Short walks (10 to 15 minutes), supported rest positions such as lying with knees bent over a pillow, and gentle position changes are appropriate. Ice if the mechanism was clearly traumatic with swelling; heat for most other presentations.
Days 4–14: Heat remains useful as a pre-movement tool. Gentle mobilization exercises — pelvic tilts, cat-camel, single knee-to-chest — work well when performed in the window of reduced spasm that heat creates. Walking duration should increase gradually. Most uncomplicated muscle-dominant lower back pain shows meaningful improvement within this window. The 7 low back pain exercises physical therapists recommend are a structured starting point for this phase.
Week 3 onward: Temperature therapy should be less necessary as movement improves and the pain-spasm cycle begins to break. Return to normal daily activities, gradually increasing load. Gym work, sport, and heavier lifting can typically resume with progressive loading rather than avoidance. If you are still heavily reliant on heat or ice at this stage, it is a good indicator that the underlying mechanism needs formal assessment.
When Conservative Self-Management Isn’t Enough
Ice and heat are tools for symptom management, not substitutes for treatment. They do not correct movement faults, address structural disc pathology, resolve nerve compression, or rebuild the stability that prevents the next episode.
Consider formal physiotherapy assessment if pain persists beyond two weeks without meaningful improvement, if you have had three or more similar episodes in the past year, if you are modifying daily activities or avoiding movement out of fear rather than physical inability, or if the pattern of your pain is unclear and choosing between ice and heat feels like guesswork.
Imaging is not routinely needed for mechanical lower back pain in the absence of red flags. An MRI or CT scan of a normal middle-aged spine will almost always show something — disc bulges, facet joint changes, mild degeneration — most of which are incidental findings that pre-date the current episode and do not change conservative management. The clinical picture, not the scan, drives the treatment decision. Imaging becomes appropriate when red flags are present, when neurological symptoms are progressive, when conservative management has genuinely failed over a reasonable period, or when surgery is being considered.
Surgery is rarely the answer for most lower back pain. For uncomplicated muscle or joint-dominant presentations, it is not indicated. It becomes a conversation when there is structural nerve compression producing progressive neurological changes — demonstrable weakness, worsening radiculopathy — that have not responded to well-delivered conservative care over three to six months. Even then, the majority of disc-related radiculopathy improves with physiotherapy and time.
Conclusion
The ice or heat for lower back pain debate has a clearer answer than the conflicting advice suggests. For the overwhelming majority of back pain presentations — guarding, stiffness, muscle-dominant aching, subacute flares — heat is the physiologically appropriate choice. It improves circulation, reduces spasm, and creates the conditions for movement and recovery. Ice serves a narrower purpose: the first 48 hours of a traumatic injury with genuine tissue damage and swelling.
Both modalities are temporary bridges, not destinations. The back recovers through movement, progressive loading, and addressing whatever mechanical factors triggered the episode in the first place. Temperature therapy, used correctly, makes that movement possible sooner. Used incorrectly, it delays the improvement that should have started days earlier.
If you’re still reaching for ice or heat for lower back pain after two weeks without clear progress, the next step is a proper assessment — not a different temperature.
Frequently Asked Questions
1. Should I use ice or heat for lower back pain right after a bad lift?
Unless you felt a clear muscular tear with immediate swelling or bruising, heat is usually the better choice even after an acute lift-related injury. Most “bad lift” pain involves disc irritation and protective muscle guarding rather than frank tissue rupture. If there is genuine swelling or the onset was traumatic enough to cause visible bruising, use ice for the first 24 to 48 hours and reassess. If it is the familiar deep ache and spasm that follows a loaded movement, heat and gentle movement are the appropriate response from day one.
2. Can I alternate ice and heat for lower back pain?
Contrast therapy (alternating cold and heat) is sometimes used in sports medicine for acute joint injuries, but for lower back pain it rarely adds benefit over heat alone. It introduces complexity without a clear physiological justification for the lumbar region. Choose based on the tissue state: ice for acute traumatic presentations, heat for everything else. If you are unsure which applies, start with heat and monitor the response.
3. I’ve been icing for several days and my back feels stiffer. What’s happening?
This is a common and predictable pattern. Sustained cold on a guarding lumbar muscle worsens vasoconstriction, deepens the ischemia driving the pain, and often increases muscle tension rather than reducing it. If ice is making you progressively stiffer rather than relieved, stop it, switch to heat, and begin gentle movement as soon as the heat has reduced the spasm enough to allow it.
4. How long should I apply heat to my lower back?
15 to 20 minutes per session is the practical therapeutic range. Beyond 20 minutes, the vasodilatory effect plateaus and the risk of mild skin irritation increases, particularly with heating pads on higher settings. Leave at least 45 minutes between sessions. The most productive use of heat is in the 20 minutes immediately before rehabilitation exercises or a walk — not as a passive pain reliever applied while sitting still for an hour.
5. Is a hot shower as effective as a heat pack for lower back pain?
Not identical, but often very effective — particularly for morning stiffness. A warm shower produces whole-body vasodilation and combines warmth with the gentle movement of positioning under the water. It will not deliver sustained localized heat to a specific lumbar segment the way a heat wrap will, but for the morning pain-and-stiffness pattern, it is one of the most clinically practical tools available and works well as a daily starting point.
6. My lower back pain radiates down my leg. Will heat or ice help?
Neither addresses the source of the problem. Leg-dominant pain suggests nerve irritation or compression at the spinal level — typically from a disc herniation or narrowing around a nerve root. Surface temperature therapy on the back may slightly reduce the muscular component of the discomfort, but it does not change the neural situation. This presentation needs clinical assessment to determine the mechanism, guide appropriate treatment, and rule out anything that needs urgent attention.
7. Can heat make lower back inflammation worse?
Heat can potentially stimulate tissue activity in an area with genuine acute inflammation, which is why it is generally avoided in the first 48 hours after a traumatic injury with swelling. For most non-traumatic lower back pain, however, there is no active inflammatory cascade — the pain is driven by muscle guarding, reduced circulation, and tissue sensitivity rather than acute tissue damage. In that context, heat is appropriate and rarely makes true inflammation worse. If you are genuinely uncertain whether your pain is acute-inflammatory or muscle-dominant, a brief physiotherapy assessment will clarify it quickly.
8. Is it normal to need heat or ice daily for lower back pain?
Daily reliance on temperature therapy beyond two weeks suggests the underlying mechanical problem is not resolving with home management. Passive symptom relief applied daily while the root cause remains unaddressed typically produces a stable-but-not-improving pattern — pain stays manageable but never fully resolves, and episodes recur. If that describes your situation, a structured physiotherapy assessment will identify what is actually maintaining the problem and give you a rehabilitation plan that targets the cause rather than the symptom.
Medical Disclaimer
This article is intended for general educational purposes only and does not constitute medical advice, diagnosis, or treatment. The information provided is based on general clinical principles for non-specific mechanical lower back pain in otherwise healthy adults and may not apply to your specific situation. If you are experiencing severe, worsening, or complex back pain — or symptoms including leg pain, numbness or tingling, bladder or bowel changes, unexplained weight loss, or fever — seek evaluation from a qualified healthcare professional. Do not delay seeking professional care based on information in this article.
References
- French SD, Cameron M, Walker BF, Reggars JW, Esterman AJ. Superficial heat or cold for low back pain. Cochrane Database of Systematic Reviews. 2006;(1):CD004750. doi: 10.1002/14651858.CD004750.pub2. PMID: 16437495.