Lower Back Pain After Bending Over: Causes, Relief, and When to Worry
“Expert Review: This article includes clinical insights from Dr. Vivek Arora, a physiotherapist with 20+ years of experience.”
Lower back pain after bending over is one of the most common ways an acute back flare starts. Sometimes it happens while lifting laundry. Sometimes while picking up a shoe, unloading the dishwasher, or reaching into the trunk of a car. The movement looks trivial, but the pain can feel dramatic.
That mismatch is what scares people. You bent for something light, but now you feel stuck, crooked, or afraid to move. In many cases, this is a mechanical low back pain episode rather than a dangerous injury. Clinical guidelines note that most acute or subacute low back pain episodes improve over time, and routine imaging is usually not appropriate when there are no red flags.[1]
Key Takeaways
- Lower back pain after bending over is often mechanical, meaning muscles, discs, joints, or surrounding soft tissues have become irritated.
- The exact pain pattern matters: pain only in the back behaves differently from pain that shoots into the leg.
- You do not automatically need an MRI or X-ray just because bending triggered the pain.
- Early management usually works better than panic, bed rest, or aggressive stretching.
- Red flags such as leg weakness, saddle numbness, bowel or bladder changes, fever, trauma, cancer history, or unexplained weight loss need urgent medical attention.

Why does lower back pain after bending over happen?
Lower back pain after bending over usually happens because bending forward places load through the lumbar discs, supporting ligaments, spinal muscles, and nearby joints. If one of those tissues is already irritated, the bend itself may be tolerable, but the return from flexion back to upright is what suddenly lights things up. Most first-time episodes are mechanical and not dangerous, and early care usually focuses on staying reasonably active, avoiding bed rest, and using simple conservative measures first.[1]
A normal bend is not supposed to come only from the low back. It should be shared between the hips, trunk, and abdominal pressure system. When the hips are stiff, the load is poorly controlled, or you bend with fatigue, twisting, or a rounded spine under load, the lower back has to do more of the work. That does not mean you have “damaged” your spine every time this happens. It means the area may have exceeded its current tolerance.
This is why two people can do the same movement and only one gets pain. The issue is rarely just the movement in isolation. It is the movement plus the state of the tissues that day: sleep, fatigue, deconditioning, recent heavy lifting, a long car ride, old disc irritation, guarding, or simply too much repeated bending in a short window.
Anatomy and biomechanics: what usually gets irritated?
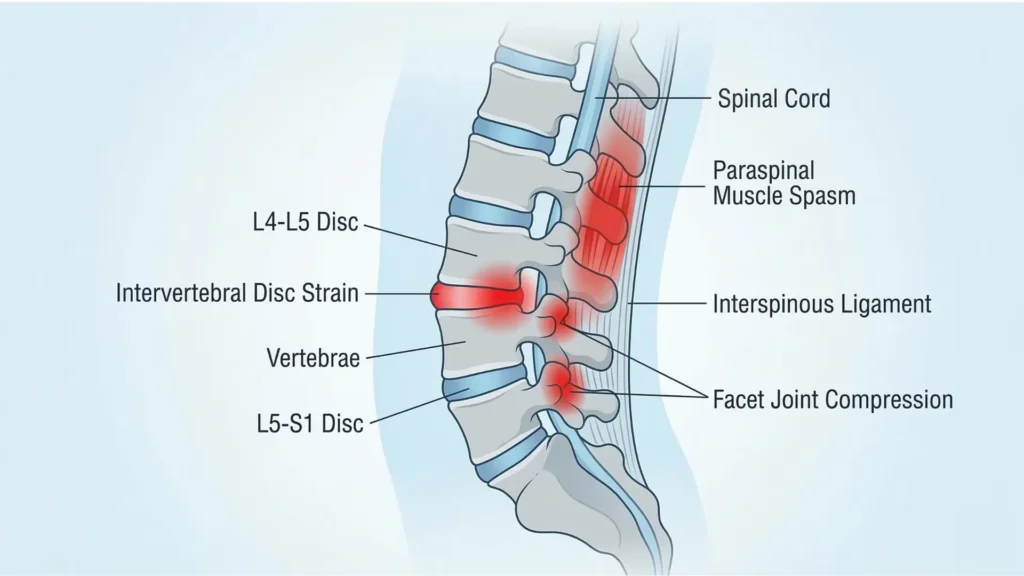
The low back is built to bend, extend, rotate a little, and transfer load between the rib cage and pelvis. The main structures that may become symptomatic after bending include:
- Paraspinal muscles and fascia: these often react with spasm or guarding after a sudden bend or awkward lift.
- Intervertebral discs: discs tolerate compression well, but repeated or loaded flexion can irritate them in some people, especially when the pain also travels into the buttock or leg.
- Facet joints: these joints usually dislike extension and rotation more than flexion, but they can still become painful after a bend because straightening back up compresses them.
- Posterior ligaments and sacroiliac-region tissues: these can be sensitive after asymmetrical bending, twisting, or reaching.
The key point is that “I bent and got pain” does not point to only one diagnosis. It is a movement trigger, not a diagnosis by itself.
Common causes of back pain after bending over
1. Muscle strain or protective spasm
This is one of the most common patterns. You bend, feel a grab, and then every movement feels guarded. The pain is usually local, sharp or tight, and worse with transitions such as sitting down, standing up, or trying to straighten fully.
2. Disc irritation
A disc-related flare is more likely when bending, sitting, coughing, sneezing, or prolonged slouching aggravates symptoms. The pain may stay in the low back, or it may spread into the buttock or leg. Not every disc flare causes sciatica, and not every bend-induced pain means a disc has herniated.
3. Facet joint irritation when coming back upright
Some people say, “Bending is okay, but straightening is awful.” That pattern can happen when the extension phase back to standing compresses already irritated posterior structures, including the facet joints.
4. Sacroiliac or posterior pelvic soft-tissue irritation
Pain near one dimple area or just off-center over the beltline can come from the tissues around the back of the pelvis, particularly after twisting while bending, carrying uneven loads, or stepping awkwardly.
5. Flexion-intolerant mechanical low back pain
This is less a single structure and more a behavior pattern. Repeated bending, slumped sitting, lifting from a rounded back, and poor hip contribution gradually sensitize the system until one ordinary bend becomes the final straw.
Symptom patterns that help narrow it down
| Pattern | What it may suggest | Common clues |
|---|---|---|
| Pain stays mostly in the low back | Muscle, fascia, joint, or localized disc irritation | Feels stiff, guarded, and worse with transitions |
| Pain is worse when straightening up | Spasm, posterior joint irritation, or disc-related guarding | You feel “stuck bent” for a while |
| Pain shoots into buttock, thigh, or below the knee | Nerve root irritation or disc-related radicular pattern | Tingling, numbness, cough/sneeze sensitivity |
| One-sided pain near the beltline | SI-region tissues, QL/paraspinals, or facet irritation | Worse with asymmetrical stance, rolling, or twisting |
| Severe morning pain plus fever, trauma, cancer history, or neurological change | Not a routine mechanical flare | Needs urgent medical assessment |
When should you worry?
Most bend-triggered back pain is not an emergency, but some situations should change the plan quickly.
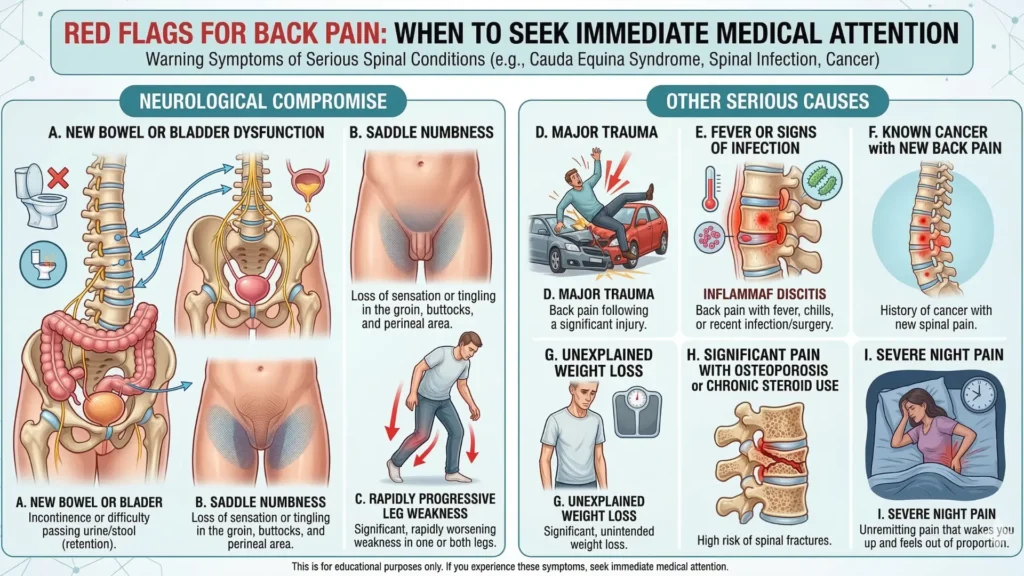
Seek urgent or emergency assessment if you have:
- new bowel or bladder dysfunction
- saddle numbness
- rapidly progressive leg weakness
- major trauma
- fever or signs of infection
- known cancer with new back pain
- unexplained weight loss
- significant pain with osteoporosis or chronic steroid use
- severe night pain that feels out of proportion
Imaging guidelines specifically escalate the workup when there are red flags suggesting conditions such as cauda equina syndrome, fracture, malignancy, or infection.[2]
Do you need an MRI or X-ray?
Usually, no.
For acute low back pain with or without radiculopathy and no red flags, the ACR appropriateness criteria list lumbar X-ray, CT, and MRI as usually not appropriate as the initial step. That is important because many people assume a painful bend automatically means they need imaging the same week. In most uncomplicated cases, that is not how good care works.[2]
Imaging becomes much more relevant when:
- red flags are present
- there is significant or progressive neurological loss
- cauda equina is suspected
- fracture risk is higher
- infection or cancer is a concern
- symptoms remain persistent or progressive after a solid trial of conservative management and intervention or surgery is being considered
The ACR guideline also notes that for patients with persistent or progressive symptoms after about 6 weeks of optimal management who may be intervention or surgery candidates, lumbar MRI without contrast is usually appropriate.[2]
A few myths worth dropping
“If I bent and got sudden pain, I must have slipped a disc.”
Not necessarily. Sudden pain can come from muscle spasm, a disc flare, posterior ligament irritation, or joint-related guarding. The movement trigger alone is not enough to label the structure.
“I should stay in bed until it calms down.”
That usually backfires. Clinical guidelines recommend avoiding bed rest and returning to normal activity as tolerated, because complete shutdown often increases stiffness, fear, and deconditioning.[1]
“Stretching hard will loosen it up.”
Sometimes it will. Sometimes it will make a flexion-sensitive back angrier. The right movement depends on what eases symptoms, what worsens them, and whether leg symptoms are appearing or spreading.
“No leg pain means it can’t be a disc.”
Not true. Disc irritation can stay local to the low back, especially early on.
From the Clinic: Dr. Arora’s Expert Insight
One pattern I see repeatedly is this: the patient blames the object or sleep. “It happened because I bent for a towel,” or “I just leaned down for my socks, or Yesterday I slept awkwardly .” In reality, the towel, or the yesterdays awkward sleep was rarely the real problem. The back was already running close to its limit, and that small bend simply exposed it.
Another mistake is going straight to generic advice. “Just stretch your hamstrings.” “Just rest for three days.” “Just strengthen your core.” Those instructions are too broad to be useful. A flexion-sensitive back does not need aggressive toe-touching on day one. A guarded, spasm-dominant back does not need a heroic workout either.
What works better clinically is sequence. First, calm the irritated pattern. Then restore confident movement. Then retrain the hip hinge, trunk control, and load tolerance that were missing when the flare happened. When people skip that middle step and jump from pain to normal lifting, the same bend tends to become a repeat offender.
What to do in the next 24–72 hours
The first goal is not to “fix” everything. It is to stop the situation from snowballing.
1. Relative rest, not bed rest
Reduce aggravating tasks for a short period, but keep moving. Short, frequent walks are usually better than lying down all day. That matches guideline-based care for acute low back pain.[1]
2. Find the least provocative position
Some people prefer lying on their back with knees bent. Others do better on their side with a pillow between the knees. Some feel best standing or walking. Your relief position matters more than internet dogma.
3. Use heat if the area feels tight or guarded
Guidelines support superficial heat as one reasonable nonpharmacologic option for acute low back pain.[1]
4. Avoid repeated painful bending for a day or two
This does not mean become afraid of bending forever. It means do not keep poking the bruise. Use a supported hip hinge, widen your stance, bring objects closer, and split the movement through the hips and knees.
5. Be careful with aggressive stretching
If every stretch reproduces the pain sharply or sends it farther down the leg, back off. Early force is often the wrong answer.
6. Use medication only if it is appropriate for you
If you and your clinician decide medication is needed, guidelines support NSAIDs or skeletal muscle relaxants in selected cases.[1]
A practical rehab progression
Phase 1: Settle the flare
Goal: reduce pain, reduce guarding, keep confidence in movement.
Examples:
- short walks
- gentle position changes every 30–60 minutes
- supported sit-to-stand
- log-roll to get out of bed
- unloaded or lightly loaded movement in the direction that feels better
A good sign in this phase is that pain becomes less intense, less sharp, and less likely to seize during transitions.
Phase 2: Restore movement quality
Goal: stop bending from happening only at the low back.
Examples:
- hip-hinge drill with hands on the hips
- chair squat or sit-to-stand
- controlled reach to a raised surface
- breathing plus abdominal brace without over-tensing
- light trunk endurance work such as dead-bug or bird-dog variations if tolerated
This is where many people realize the issue is not “weak core” in the vague social-media sense. It is poor load sharing between the hips, trunk, and back.
Phase 3: Rebuild load tolerance
Goal: return to real life.
Examples:
- picking an object up from a low box before going to floor level
- split-stance lifting practice
- glute bridge and hip-dominant strength work
- farmer carry variations
- return to gym lifts with reduced load and stricter mechanics
The test is not whether you can do one perfect rep in a rehab session. The test is whether you can repeat normal life without the back tightening every time.
Do’s and don’ts
Do
- keep moving within a tolerable range
- change positions often
- use the hips more when you bend
- keep objects close to your body
- get assessed sooner if pain is going into the leg or weakness is appearing
Don’t
- stay in bed for days
- repeatedly stretch into sharp pain
- panic and assume the worst from one painful movement
- jump straight back to heavy lifting the moment the pain drops
- ignore red flags because “it’s probably just a pulled muscle”
Return to exercise, work, and normal life
A desk worker may need better sit-to-stand frequency and a cleaner hinge when reaching down. A parent may need a new strategy for picking up a child. A gym-goer may need to temporarily reduce deadlift or row volume and rebuild from a shorter range. The principle is the same: return early, but return intelligently.
You do not have to wait for pain to reach zero before doing useful activity. You do need the activity to be dosed well enough that you are not worse the next day.
When conservative care is failing
Get reassessed if:
- the pain is not clearly improving over 1–2 weeks
- you repeatedly get “stuck” after minor bends
- leg pain, tingling, or numbness is becoming more dominant
- walking tolerance is shrinking
- you cannot return to basic daily function
- weakness is appearing
Surgery is not the routine answer for a simple bend-and-pain episode. It becomes a more serious discussion when there is a major neurological problem, a surgical emergency such as cauda equina, or persistent or progressive symptoms where imaging and the clinical picture line up after appropriate conservative care. The ACR criteria specifically escalate MRI in patients with persistent or progressive symptoms after about 6 weeks when intervention is being considered.[2]
What is the outlook?
The outlook is usually good. Most acute and subacute low back pain episodes improve over time, especially when people avoid bed rest, stay reasonably active, and address the movement pattern that triggered the flare. The catch is recurrence: pain calms faster than capacity rebuilds. If you only wait for symptoms to settle and never retrain bending, lifting, and trunk control, the next awkward reach may restart the cycle.[1]
Conclusion
Lower back pain after bending over is usually a mechanical flare rather than a sign that your back is permanently damaged. The real job is to read the pattern correctly: local spasm behaves differently from leg-dominant nerve pain, and a routine strain behaves very differently from a red-flag presentation. Calm it down, keep moving, rebuild the hinge, and get assessed sooner rather than later if the symptoms are severe, spreading, or neurologically concerning.
FAQs
1. Can bending over cause a slipped disc?
Yes, bending can trigger a disc-related flare, but it is not the only explanation. Many cases of pain after bending come from muscle spasm, soft-tissue irritation, or joint-related guarding. The presence of leg pain, tingling, numbness, or cough/sneeze sensitivity makes a disc pattern more likely.
2. Why does my back hurt more when I straighten up than when I bend?
That often happens because returning to upright loads irritated tissues differently than the bend itself. Muscles may spasm, discs may feel compressed differently, and posterior joints can become painful as you extend back to standing.
3. Should I stretch my hamstrings if my lower back hurts after bending?
Not automatically. If your back is flexion-sensitive, aggressive hamstring stretching can worsen symptoms. In the early phase, it is usually smarter to choose movements that reduce pain, improve confidence, and restore a clean hip hinge instead of forcing range.
4. Is heat or ice better for this kind of back pain?
Heat is often more helpful when the back feels tight, guarded, or spasm-prone. Ice can feel good to some people, but acute low back pain guidelines specifically support superficial heat as one reasonable conservative option.[1]
5. When should I get an MRI for back pain after bending over?
You should not usually rush to MRI for a first uncomplicated episode. Imaging becomes more appropriate when red flags are present, neurological deficits are progressing, or symptoms remain persistent or progressive despite a good conservative trial.[2]
6. Can I walk if my lower back hurts after bending over?
Yes, usually. Short, tolerable walks are often better than prolonged bed rest because they reduce stiffness and help maintain normal movement. If walking sharply worsens leg pain or weakness, that changes the picture and you should be assessed.[1]
7. How long does a bend-related back flare usually last?
Many mild-to-moderate mechanical flares begin settling over days to a couple of weeks, though full confidence with bending can take longer. Guidelines note that most acute or subacute low back pain improves over time, but recurrence is common if movement capacity is not rebuilt.[1]
8. Should I avoid the gym completely?
No, but you should modify it. Early on, reduce painful bending and heavy axial loading, then rebuild with cleaner technique, smaller ranges, and lower loads. A temporary regression is usually smarter than either total shutdown or trying to prove you are “fine” too soon.
Medical Disclaimer
This article is for educational purposes only and does not diagnose or replace individual medical care. If you have severe pain, trauma, fever, cancer history, bowel or bladder changes, saddle numbness, progressive weakness, or symptoms that are worsening rather than settling, seek urgent medical assessment.
References
- Qaseem A, Wilt TJ, McLean RM, Forciea MA, et al. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2017;166(7):514-530. doi:10.7326/M16-2367.
- Hutchins TA, Peckham M, Shah LM, et al. ACR Appropriateness Criteria® Low Back Pain: 2021 Update. J Am Coll Radiol. 2021. PMID: 34794594.



